


When and How Can Vaccine Particles Hurt You? - A Visualisation Exercise
The Bolus Theory details out the mechanism of harm of inadvertently injecting a cytotoxic product intravascularly: vaccines, venoms, toxins...

In this article, I attempt to give a wholistic view on the processes by which adverse effects happen in the hope that it will help as many people as possible address jointly with their physicians their vaccine-induced illness.
This week has been particularly difficult for me as the more I re-engage with my friends and the world, and the more I see the damage done by these successive immunisation campaigns.
To this day, I count around me at least 16 people hurt: 5 died of which 2 were healthy and < 65, 3 had strokes, 2 had to have their heart operated… it’s a mess. I am convinced many more have been hurt around me, but the vast majority are blind to the reality that they have damaged their body and that there’s no turning back.
Tuesday night, I had a nice one-on-one dinner with an old friend in Paris. We hadn’t spoken seriously in a long time. When we last spoke, I had sensed that he had been injured by the vaccine. But - like everybody else - my brain had dismissed that thought … anything to get away from more stress and anguish.
As we progressed through our conversation, I learnt that in the past 18 months, he had lost 30% of his lungs, had needed an emergency heart operation to extract a blood clot, and that his gallbladder was now entirely dysfunctional and needed to be removed … doctors gave him absolutely no explanation! Not one single hypothesis. Grrr…
It’s saddening and infuriating for me to have failed at preventing most of my friends and a great many of my loved ones from these shots. Identifying now signs of vaccine injury on them makes for a sad look on someone one loves…
Having done a year-long deep-dive in the epidemiology and immunology of the SARS-Cov-2 epidemic, mid-January 2021, it was evident to me that these vaccines were seriously hurting people. One could see that something was seriously wrong in the overnight - New Year’s Eve - instantaneous reversal of the COVID death curves: that was an epidemiological impossibility! COVID deaths had been falling since mid-November, a sign Susceptibles were depleted. Immunocompromised Susceptibles simply can’t be created overnight. And the variant narrative was easy to dispel for my friend Mike Yeadon and I. The synchronicity of this renewed COVID death momentum, synchronous with the rapid implementation of vaccines, was a clear red flag. This all didn’t make sense. The vaccination was causing harm in a grand scale.
To the exception of Dr. Roger Hodkinson, Dr. Mike Yeadon and a few others, most of my fellow Panda members were in denial. Our exchanges were quite emotional, non scientific and quite frankly frustrating. On the one side, some of us were projecting the disaster unfolding, and the moral weight on our shoulders was crushing. And on the other, understandably and quite naturally, many had vaccinated their families and the slightest doubt on the innocuity of the vaccination wasn’t acceptable to their psyche. The sad perspective was too heavy to bear for many: people don’t want to know the future, and certainly not if they’ve inadvertently poisoned their kids, or their parents. We’ve been fighting this paradox ever since. Worse, once hurt, many people become even more dependent on the healthcare system, and sadly doubting isn’t even an option for them to consider.
I won’t mention the immense societal pressure we all faced, and still face. Doubting vaccines was more than sinful and the risk was - and still is - modern-day excommunication. A whole civilisation like a drowning man panicking who ends up beating and drowning the life-guard who came to save him…
In the end, I don’t think I ever convinced anyone. The reality finally caught up to the vast majority of Panda members some eight or nine months later, better than most… now it’s a reality to all of them. Frustrated, stressed, lonely, I dove into the science, into root cause analyses, into visualising what was happening with these vaccines particles. I met Steve Kirsch and another team of wonderful people, Dr. Jessica Rose, Dr. Byram Bridle, Dr. Peter McCullough, Matthew Crawford … who early had opened their eyes to this living nightmare.
Having worked for a company who had developed 2 anti-cancer therapeutic vaccines, visualisation of cells1 “infected” by cancer and the dynamics of immune cells was second nature to me… I just needed to work, observe the data, question the facts, get more data, draw more hypotheses, and validate or invalidate them. That’s what I do for a living as a consultant, and here is where that process and hard work has brought me today. The understanding of how these vaccines are hurting people. Get ready for a morbid deep dive.
Why the Bolus Theory stands
Many of my friends tell me: “Marc, there has to be more to it than your theory” as if that statement were a scientific certainty. They might well be right, but the Bolus theory stands firmly and explains most - if not all - the injuries observed. Nearly all steps in the theory detailed herein are either proven or confirmed indirectly. Hardly any conjecture. It is noteworthy to remember that the Bolus Theory is:
Factual: Inadvertent intravenous injections are a clinical reality in many fields.
Dentists2 know full well about that risk with anaesthetics, and use the aspiration technique daily to avoid accidents.
Plastic surgeons3 also know the risk of injecting hyaluronic acid fillers accidentally intravenously4.
Anesthesiologists5 equally know that risk, notably for epidural injections.
So do bodybuilders with steroids.
Accidental intravascular injections are well documented and lead to numerous pathologies like gangrene6, heart failure, blindness…similar to many adverse effects we are witnessing today, even with other products.
Consistent with existing practices in medical and drug delivery:
as early as 1936, accidental IV injection have been known to cause allergic shocks7.
the sheer existence and the past wide adoption of “the aspiration technique” demonstrates vividly the reality of that risk.
to deliver rapidly a drug to the heart or other organs, the medical profession doesn’t use a saline bag, it creates a bolus via a rapid intravenous injection.
Material:
In dentistry: aspiration proved positive in 4% of cases8 in nerve block procedure, and in 11% of mandibular blocks!
In bodybuilding: 2% of steroid injection - despite aspiration ! - were intravascular9.
Many observations have shown that numerous injections are not done according to the procedure. They are often inserted below the safe zone10, or with an angle that can hit sub-cutaneous veins11.
Another study showed that many high BMI patients have a significant risk of coming short.
Founded on robust and validated scientific realities:
the large physiological presence of blood vessels in the Deltoid

the proven fluid dynamics of bolus and dilution in the blood stream
the transfecting reality of lipid nanoparticles
the inevitability and the demonstration of the immune reaction12 to and destruction of cells expressing foreign antigens13
the activation of platelets14 following intravenous injection of adenovirus15 vectors
the vaccine has been found to cause permeability in the heart’s endothelium16
Indirectly Consistent:
Many victims of AEs testified of a metallic taste in the mouth17 immediately after the injection ( How could it get there so quickly other than by the blood stream? ). When bodybuilders get Tren Cough18, they also get a taste in the mouth, apparently a spicy one...
Other vaccines that penetrate cells with antigen - like attenuated virus vaccines (MMR, smallpox, chickenpox, yellow fever…) - also seem to have significant adverse effects. In other words, this isn’t specific to COVID vaccine technologies. A 2015 study 19 showed that the smallpox vaccine had 10.6% adverse effects, whereas the non-transfecting Influenza vaccine had 2.6% with zero severe AEs. In other words, we’ve never vaccinated so many people in so little time, and we got to see damage hidden in plain sight for decades, explaining many current illness notably neurodegenerative diseases20.

Chart 1 - Comparison of AEs between the SmallPox (SPX) and Influenza (TIV) Vaccines Accidental intravascular injection of a toxin bolus21 - such as hyaluronic acid fillers - does similar endothelial apoptosis and also causes vascular occlusion, necrosis, blindness etc…
Clinically Consistent: In line with the injuries and symptoms of these adverse effects as you will see in the coming lines.
Addendum January 2023:
Last December, I found two studies22 that demonstrate that experienced nurses - even when they aspirate - end up inadvertently to inject directly in the circulatory system 1.9% of the time. Read “Another One Bites The Dust”What is the Unified Bolus Theory?


Most of my readers have a pretty good sense of my theory23 by now. But today I will dive deeper to explain how it is that adverse effects are so diverse in severity, in symptoms and in location, and how it is mostly physics - concentration, dose, time, location - that explains it all, not micro-biology, even though of course the mechanism of harm is indeed the immune attack of any cell penetrated by a vaccine particle to bring - or create - a very immunogenic antigen (aka foreign material viewed by the immune system as a threat that needs to be destroyed) inside healthy cells.
The Spike protein is the antigen that triggers these immune attacks, and the same effective immunological processes that occur with suppressing a viral infection, destroy both transfected cells (Ts + NKs) and circulating spike proteins (That’s what antibodies are for!). I have already written an article about24 the fact that the problem isn’t the circulating spike. Traces of circulating spike proteins do not constitute a proof of much of anything, and I have yet to see any analysis showing pathological quantities.
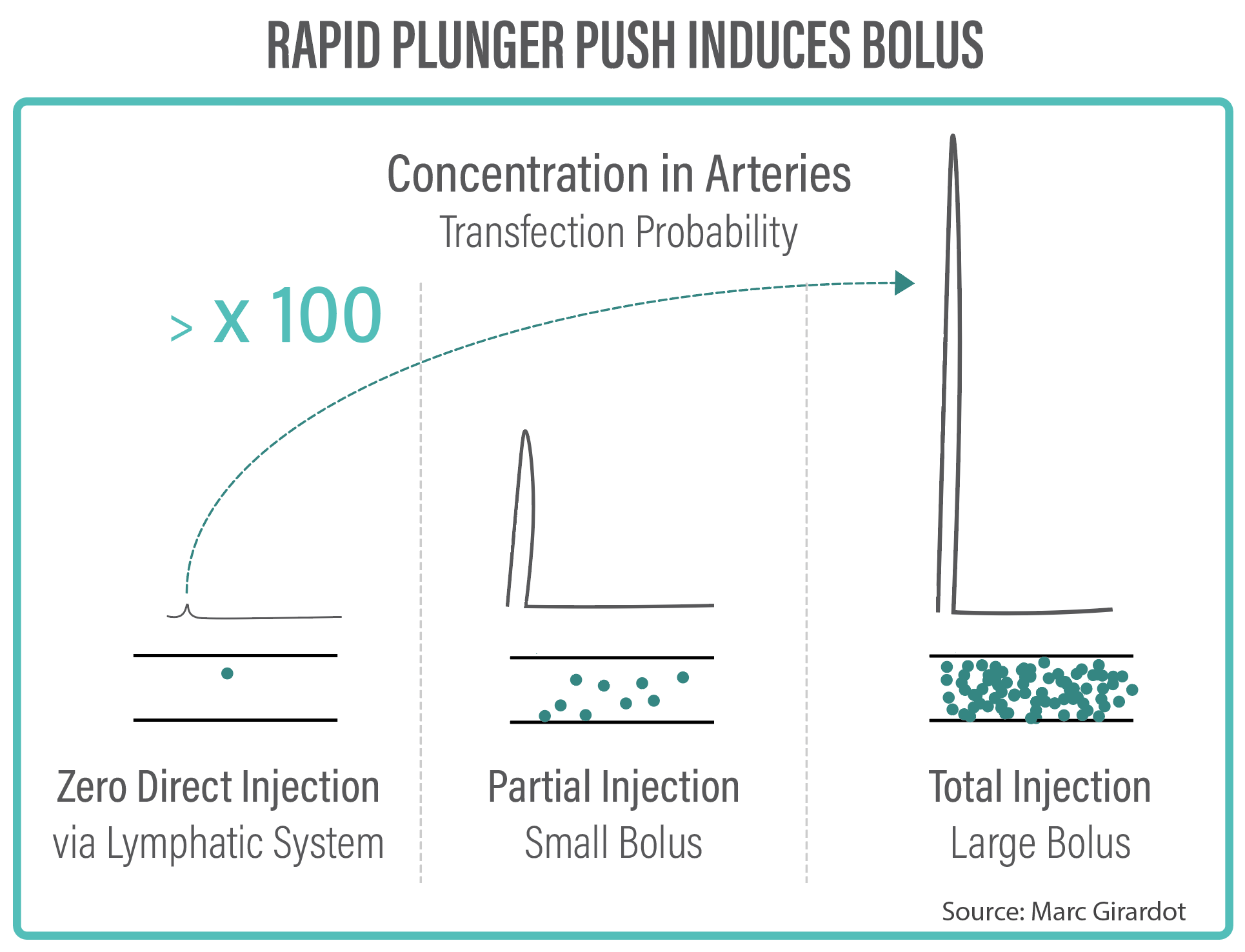
So here we go! Chart 2 is a high-level view of the dynamics of harm of any transfecting vaccine injected intravascularly (or any toxin injection for that matter).
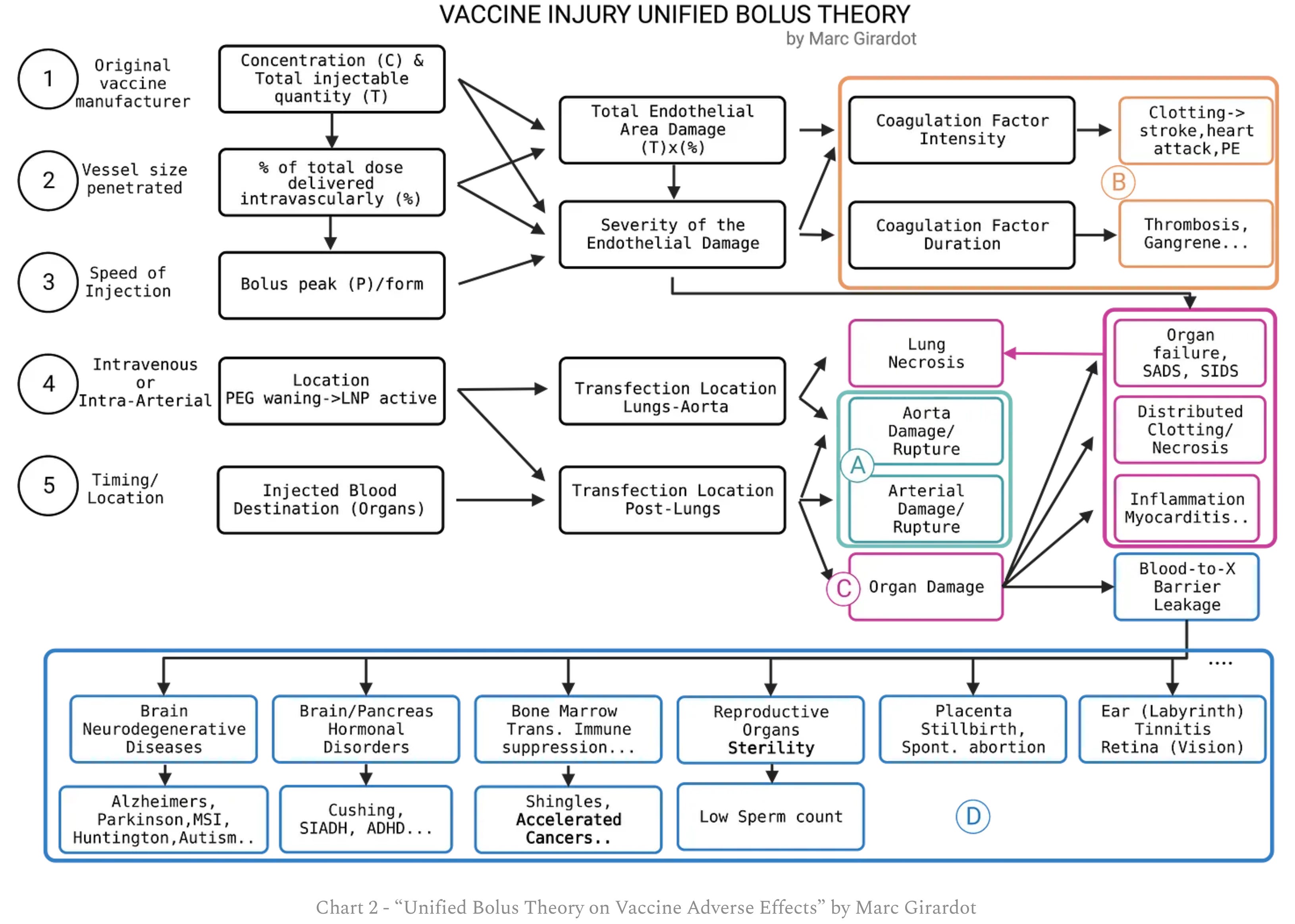

As you can see there are essentially 5 main drivers of adverse effects:
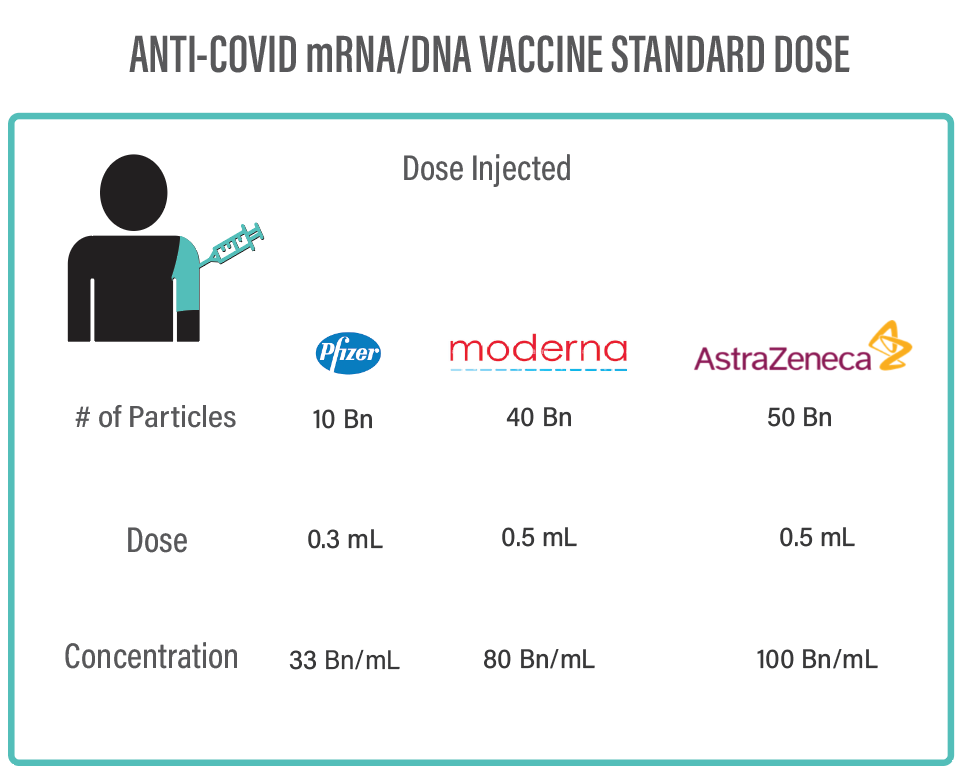
The concentration and the total dose of the vaccine chosen is the baseline. The larger the dose and the concentration, the higher the transfection potential, and the possibility of harm. A bolus created by the Moderna vaccine is 2.4 x more concentrated than Pfizer’s25, and will last somewhat longer given it has 4x the number of transfecting particles. That explains why Moderna and AstraZeneca seem to have relatively higher AEs.

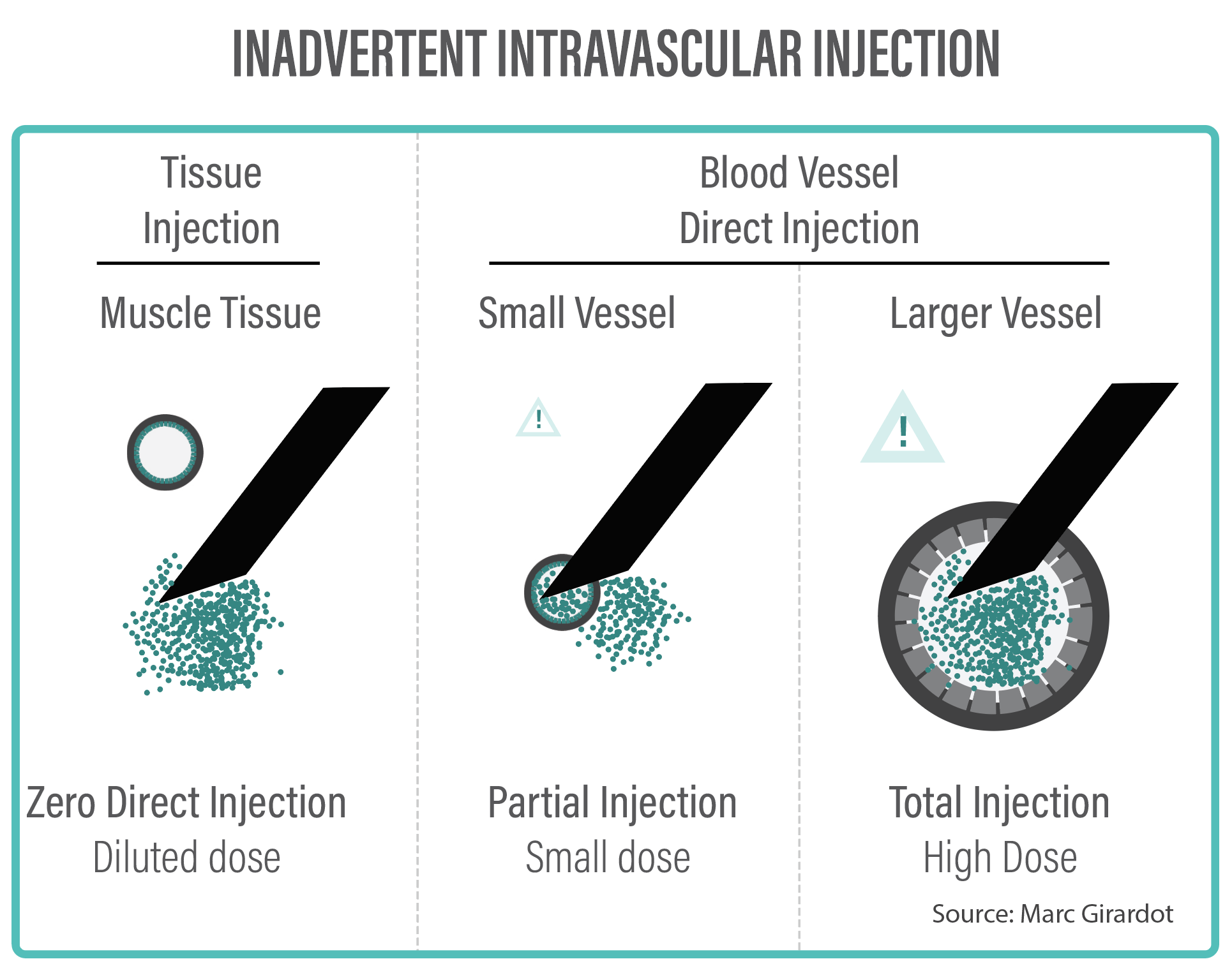
The capacity to create a Bolus emerges from an intravascular injection. We have outlined above that inadvertent IV injection is a much more common event than what most doctors think. Given the hyper-vascularisation of muscles, but also the proximity of sub-cutaneous veins, it is not surprising that many accidents occur, notably with untrained personnel.

In some instances, the needle might hit a small vessel and only inject a fraction of the standard doses. In other cases, a large portion, if not the entire dose, might be injected, leading to a much greater transfection potential of the endothelial linings of the blood vessels. We know this is real and material for the COVID vaccine, just as it is real for other vaccines and other medical procedures.
Intravenous drugs (antibiotics26, anti-inflammatory…) that need to be distributed throughout the body are typically injected very slowly, often over 2 to 5 minutes. Other drugs or products that need to be delivered concentrated into organs are delivered intravenously with a rapid push on the plunger to create a bolus in the blood stream, and deliver a concentrated dose to the organ.
COVID vaccine protocols - as many other vaccine protocols - recommend to inject the product in one rapid push. If in a blood vessel, that would necessarily create a Bolus, the concentration and the size of which would be dependent on the % of the standard dose that got effectively injected.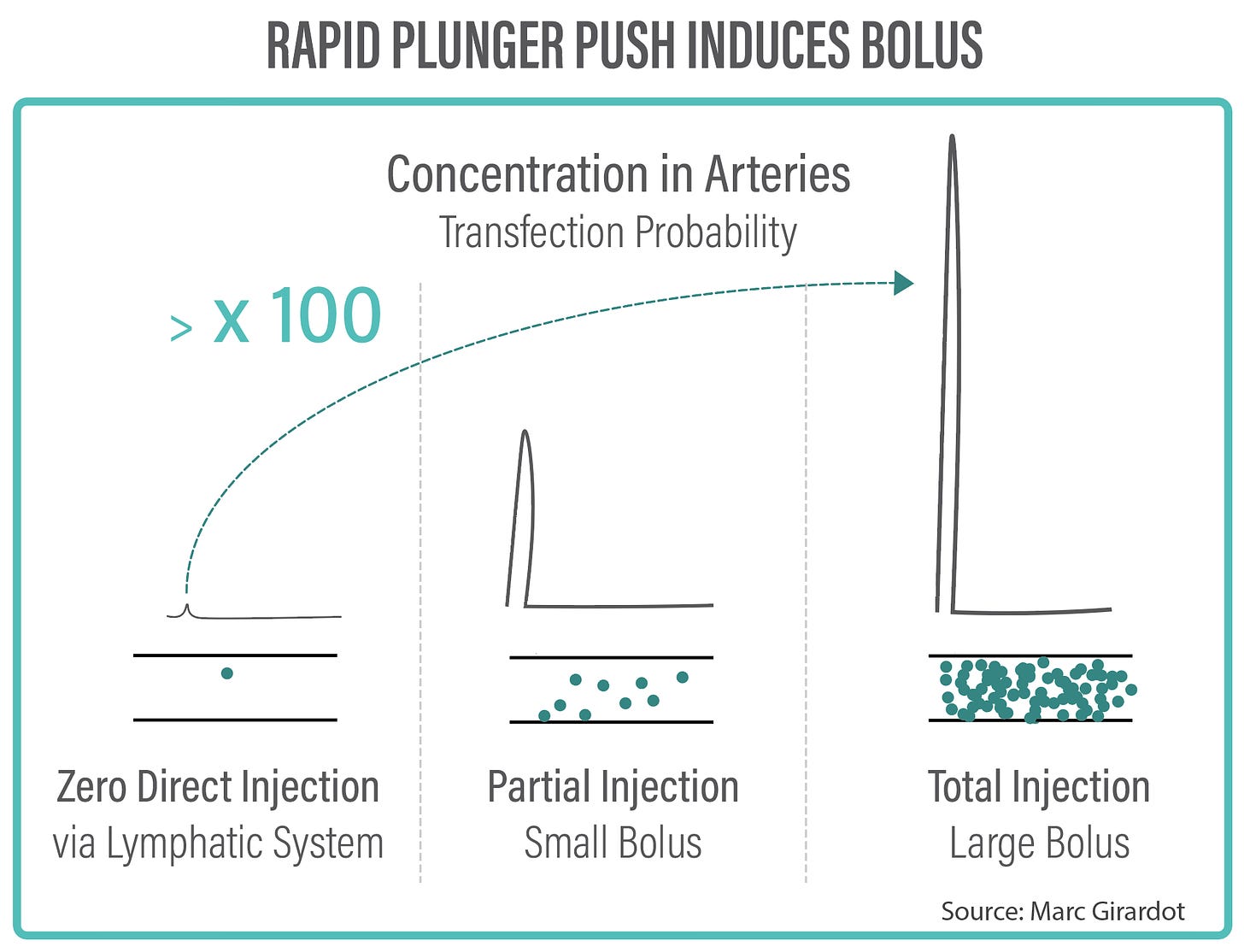
During this brief Bolus phase, these billions of circulating transfecting vaccine particles - Lipid nanoparticles, viral vectors, or attenuated viruses - mostly stuck in the vascular system will end up transfecting with varying degrees of concentration. And every single cell identified by the immune system as compromised will be destroyed.

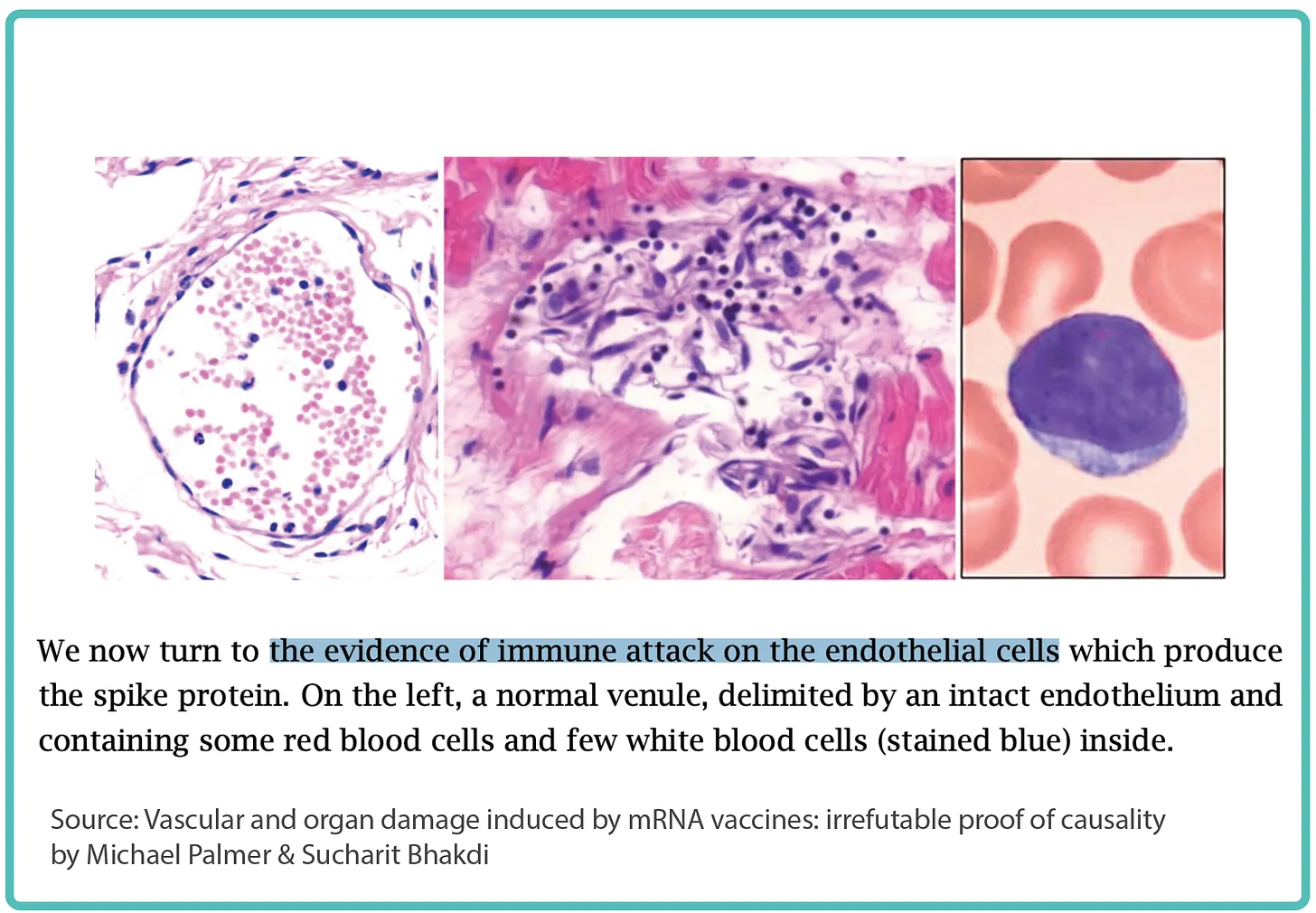
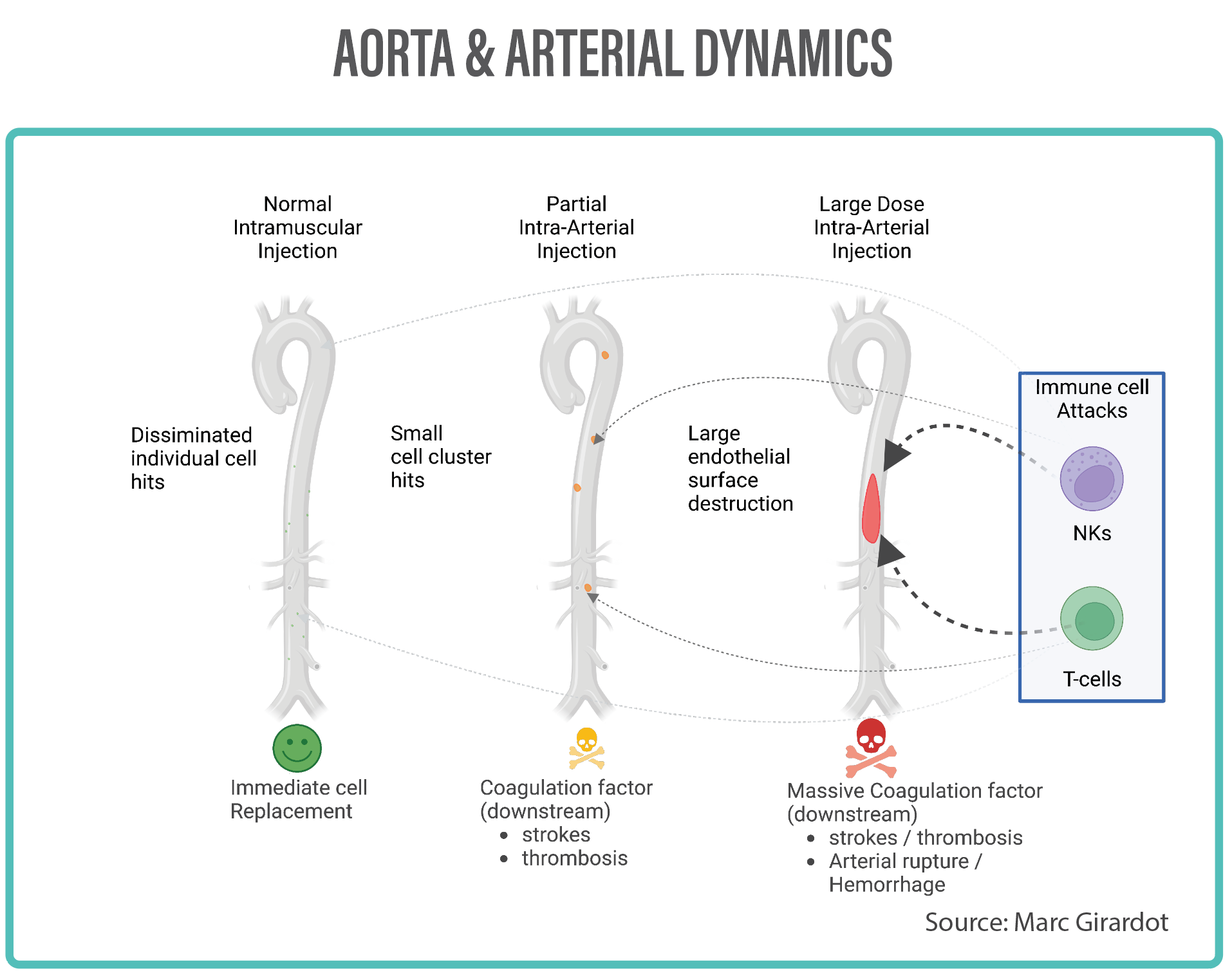
Endothelial stripping and destruction of a small vessel after vaccination
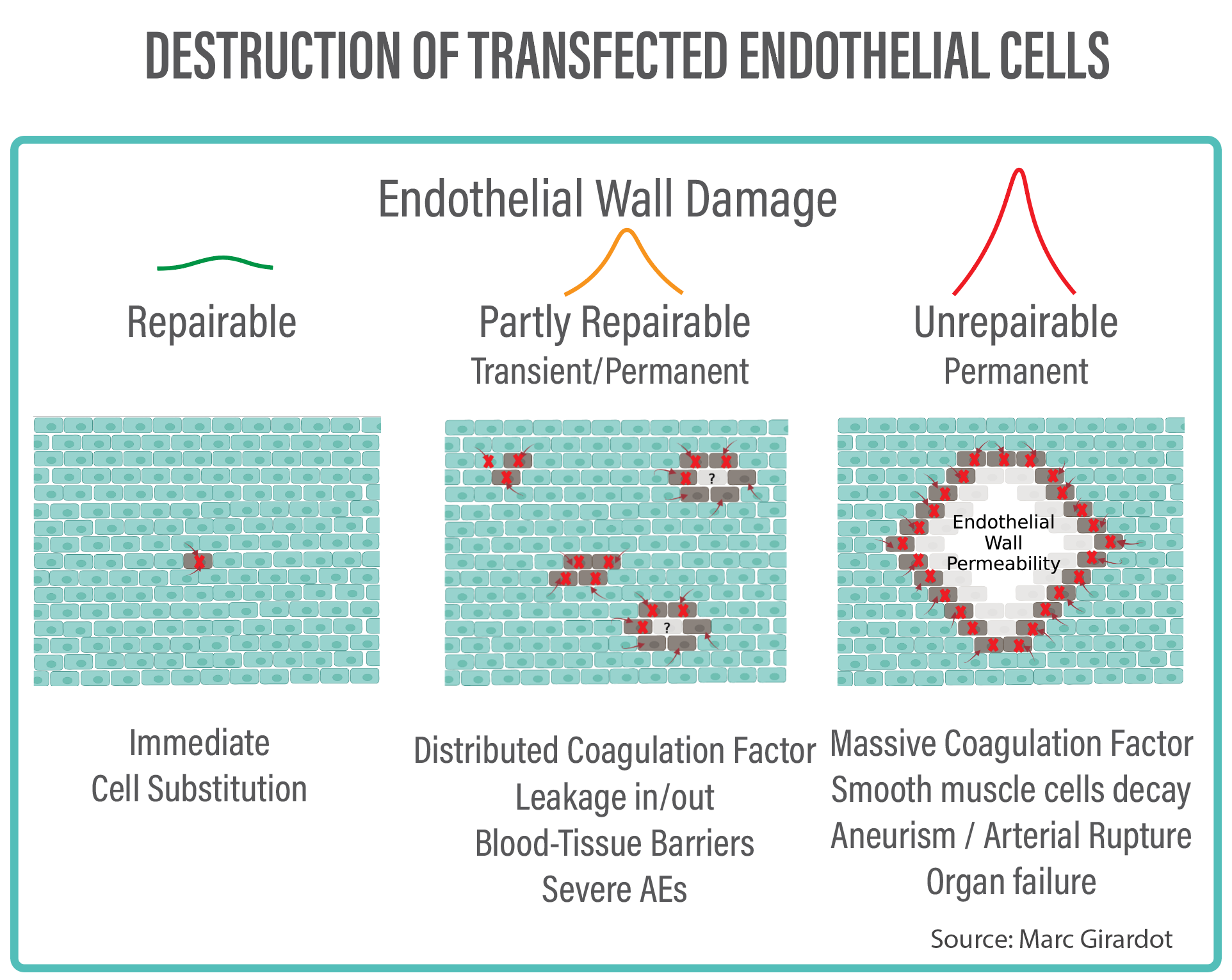
When the immune hit is one single cell, a neighbouring cell will duplicate to replace the missing cell, and the endothelial wall will repair perfectly. When multiple cells are hit simultaneously in a concentrated fashion, the natural process of repair no longer works. Anyone having suffered a large third degree burn will know the standard healing process no longer works. In the best case, the endothelial wall function can be limited. In the worse case, a deleterious process is triggered with the smooth muscle layer being unprotected and decaying, leaving the elastin layer bare, subject to crystals and fibrins, and later leading to arterial rupture, haemorrhage and death.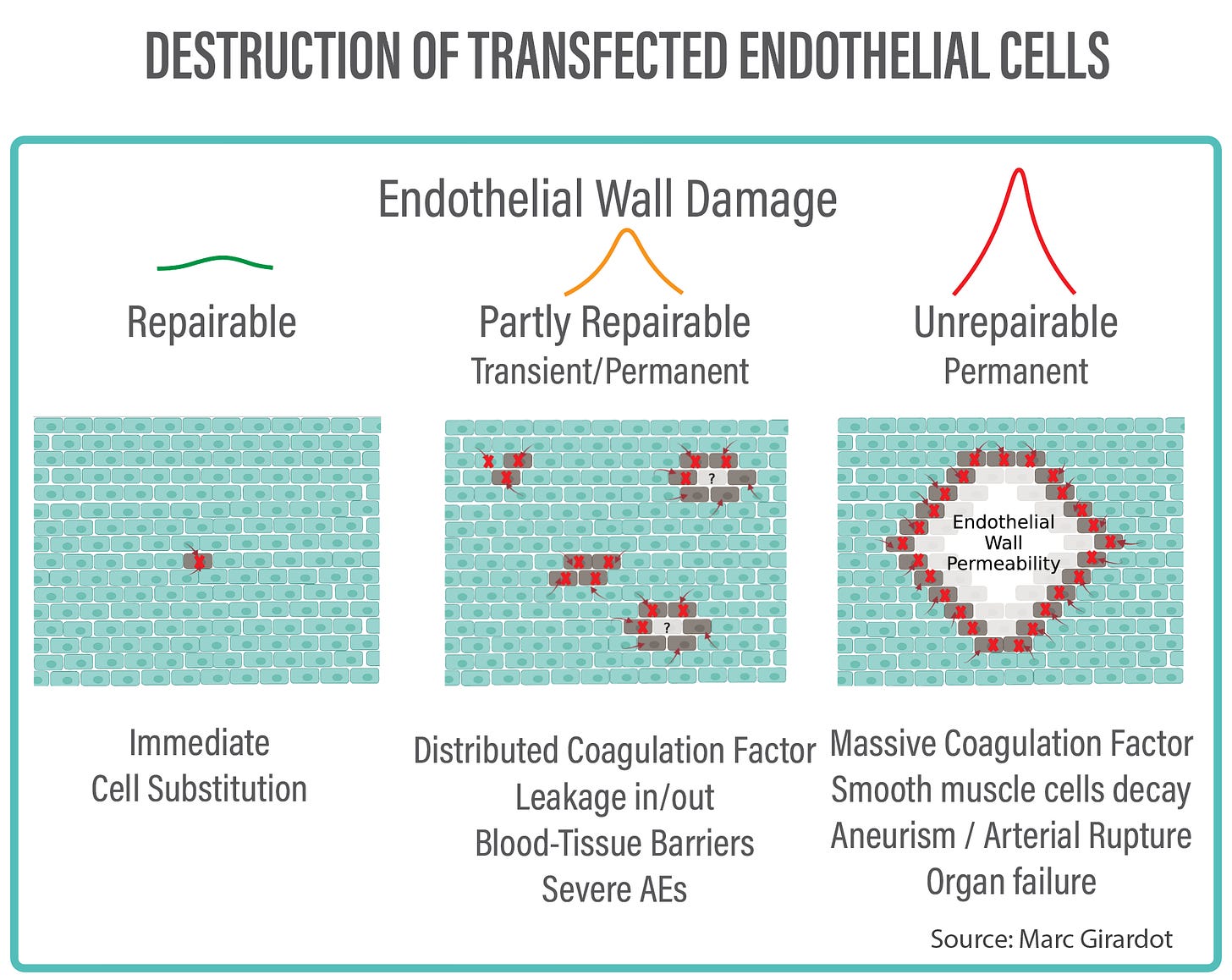
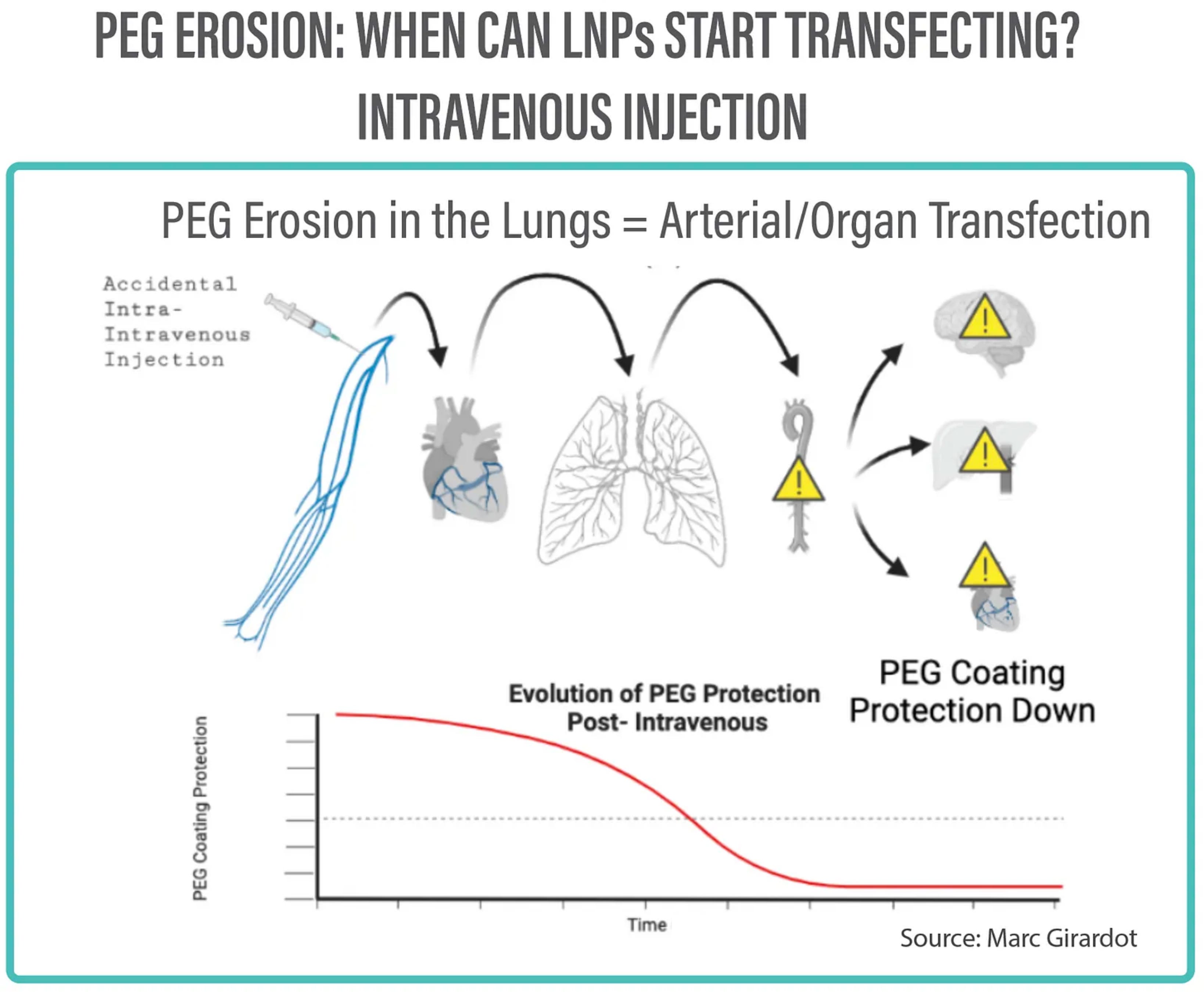
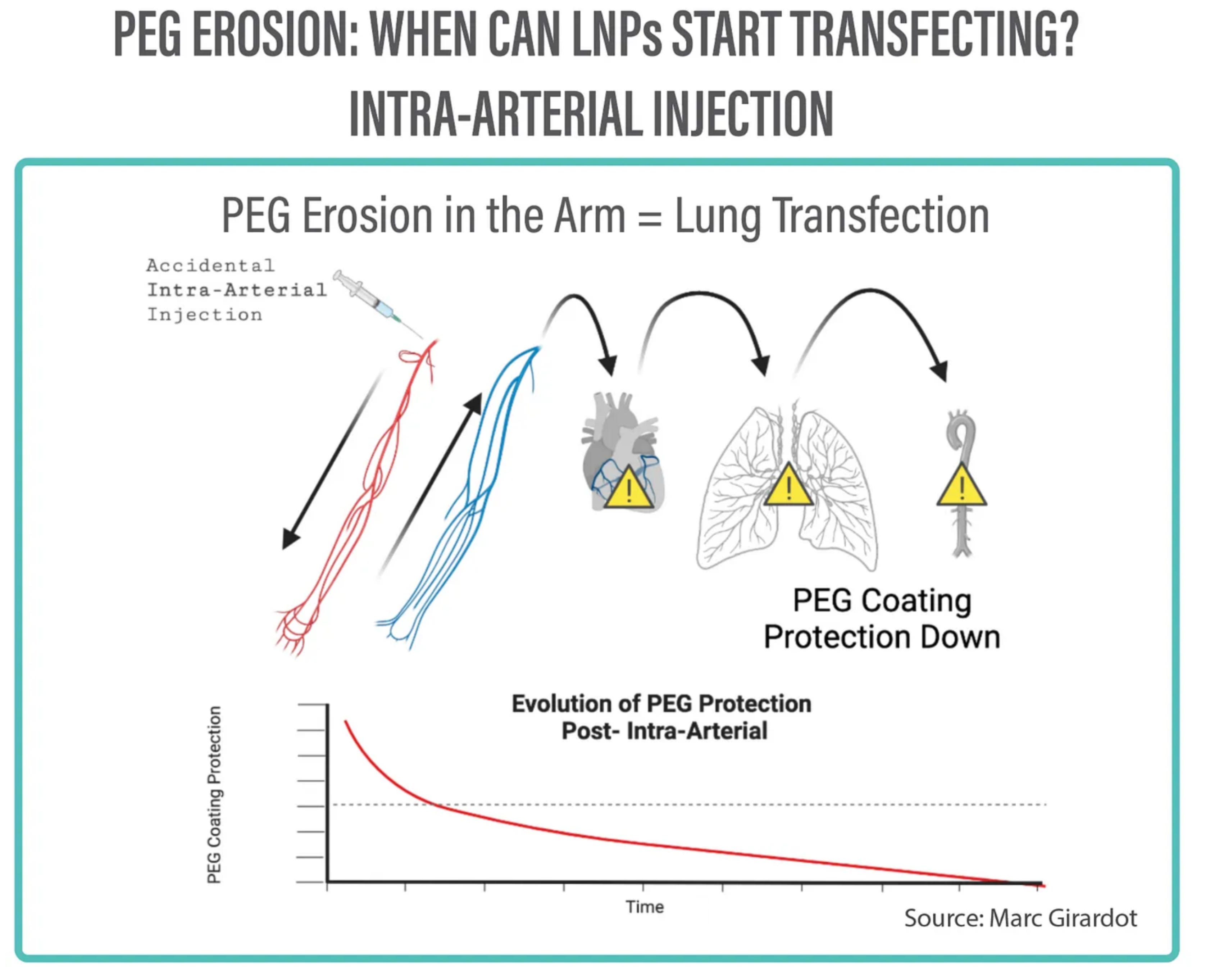
For storage and protection purposes, vaccines particles are coated with PEG (PolyEthylene Glycol) which avoids their aggregation into one big lipid bubble.
In the first instant, this coating impedes any transfection. It is likely after a few instants that the coating rubs off, and that the lipid nanoparticles can be active and transfect.
Simultaneously, the dose starts diluting itself into the blood. The more diluted, the less dangerous. Ideally, one would have designed a slow rubb-off coating to guarantee for dilution, and safety against concentrated transfection…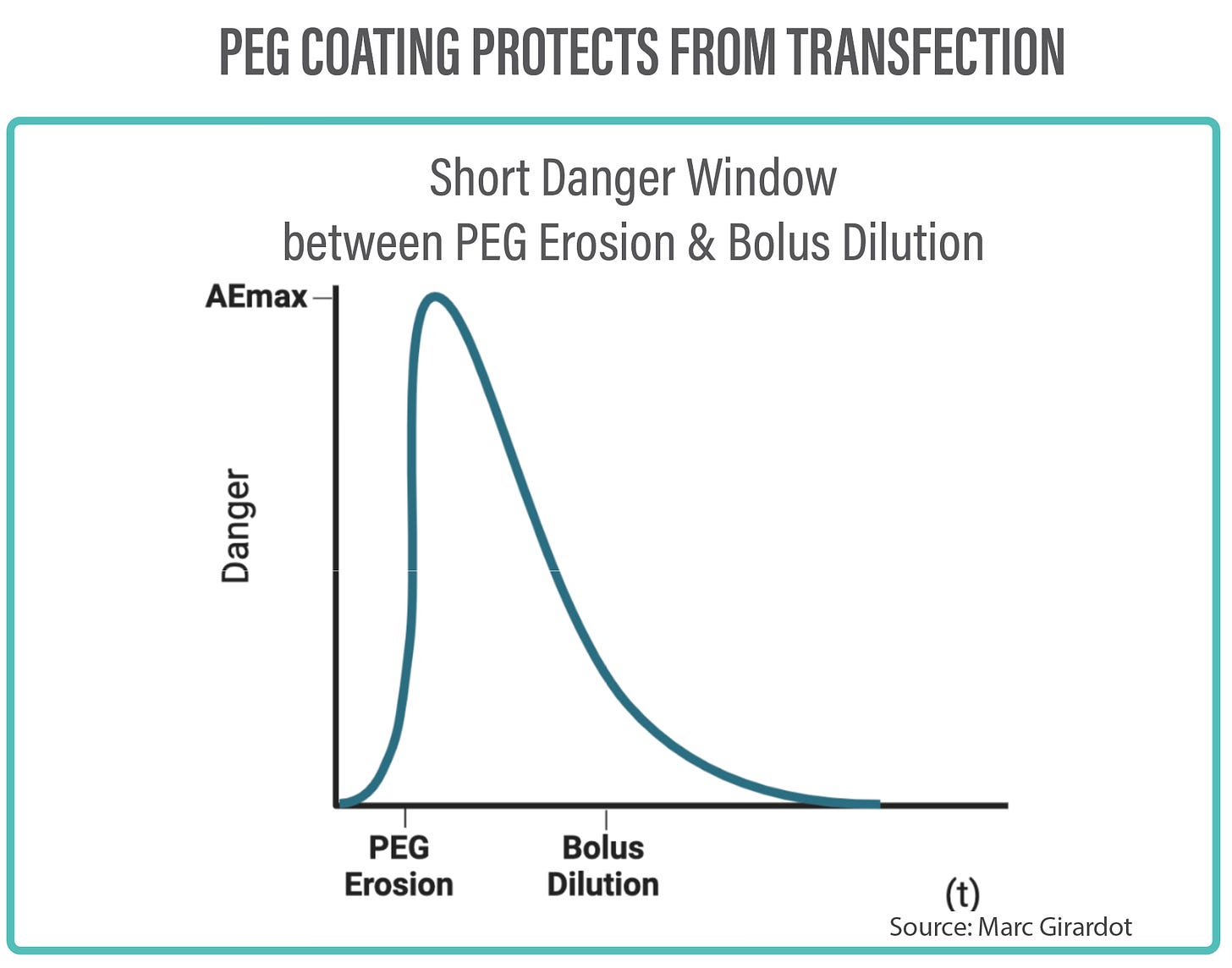
One needs to visualise the place of intravascular injection and a minimum distance of LNP circulation in the body before transfection is active: the time and distance necessary for rubbing off the coating bouncing inside the blood stream. If the injection in the Deltoid is intravenous, the bolus will go to the heart and immediately to the lungs, likely losing the protective coating through the pulmonary capillaries, and only have significant transfection potential outside the heart into the aorta and the arterial system.
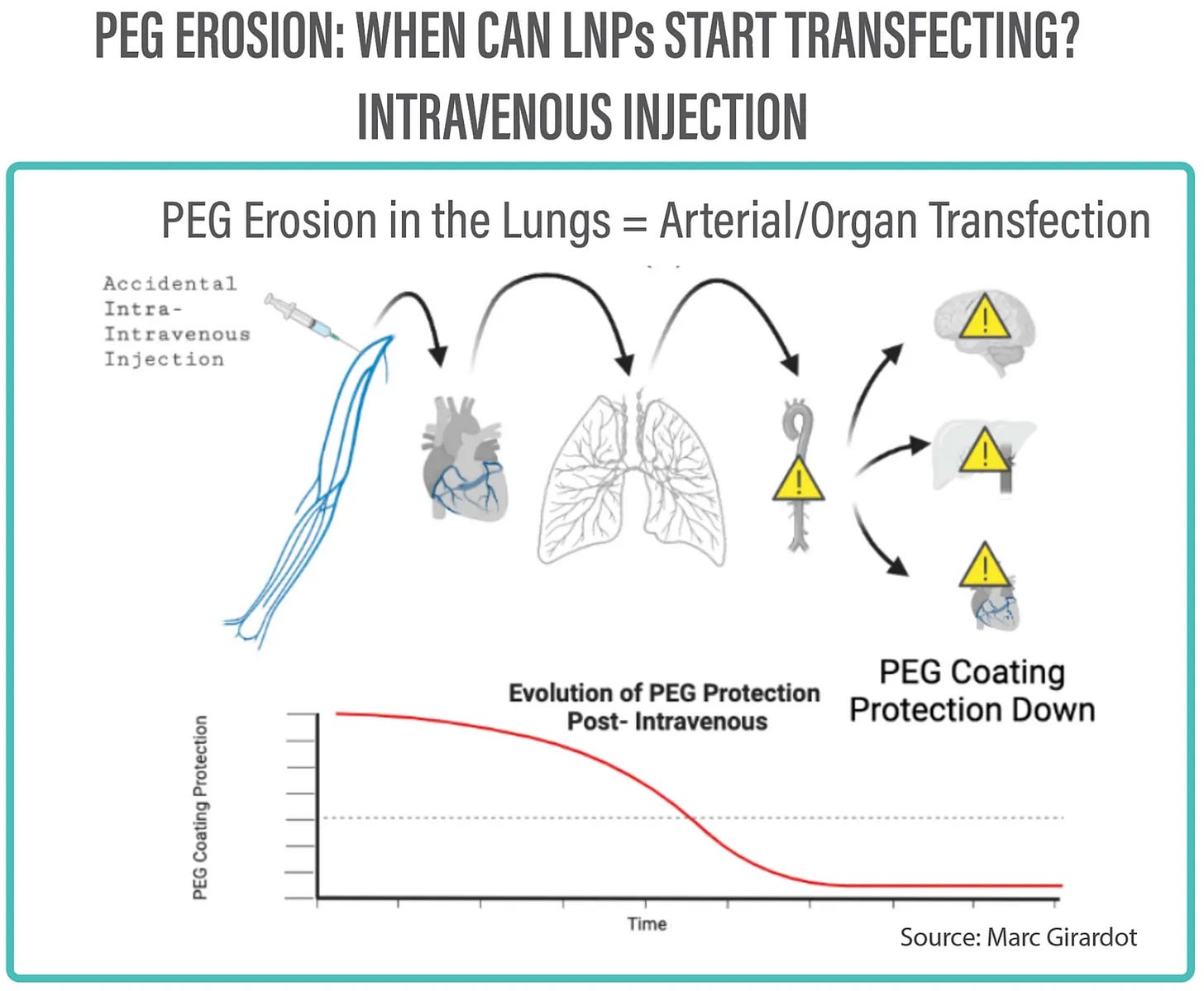
But then how did my friend lose 30% of his lungs? By the time the bolus circulates back it probably has been diluted and has transfected the organs?
Well, one needs to consider the possibility of intra-arterial injection, which makes for a longer two-way journey through the arm and hand capillaries, activating the LNPs to transfect the lungs and the aorta in a concentrated manner.…
What happens when a bolus of active LNPs exits the heart and is pumped under pressure into the aorta and the arterial system?
Well, the higher the LNP concentration, the higher the transfection rate. If a large area is hit by nanoparticles, the immune system will come swopping in and will literally wipe out the endothelial wall, stripping part of the lining of the Aorta.
This in turn will kick start two processes:
- an ineffective coagulation process stimulated by the destruction of the lining and rendered useless by the combined size and pressure of the arteries. A process that produces clots that are carried downstream in large quantities risking thrombosis further down in the capillaries and the veins. This is only normal as a cut in the lining is what normally triggers coagulation.- a deleterious process of the artery with the long exposure to the bloodstream of the smooth muscle cell layer, leading to collapse and rupture.

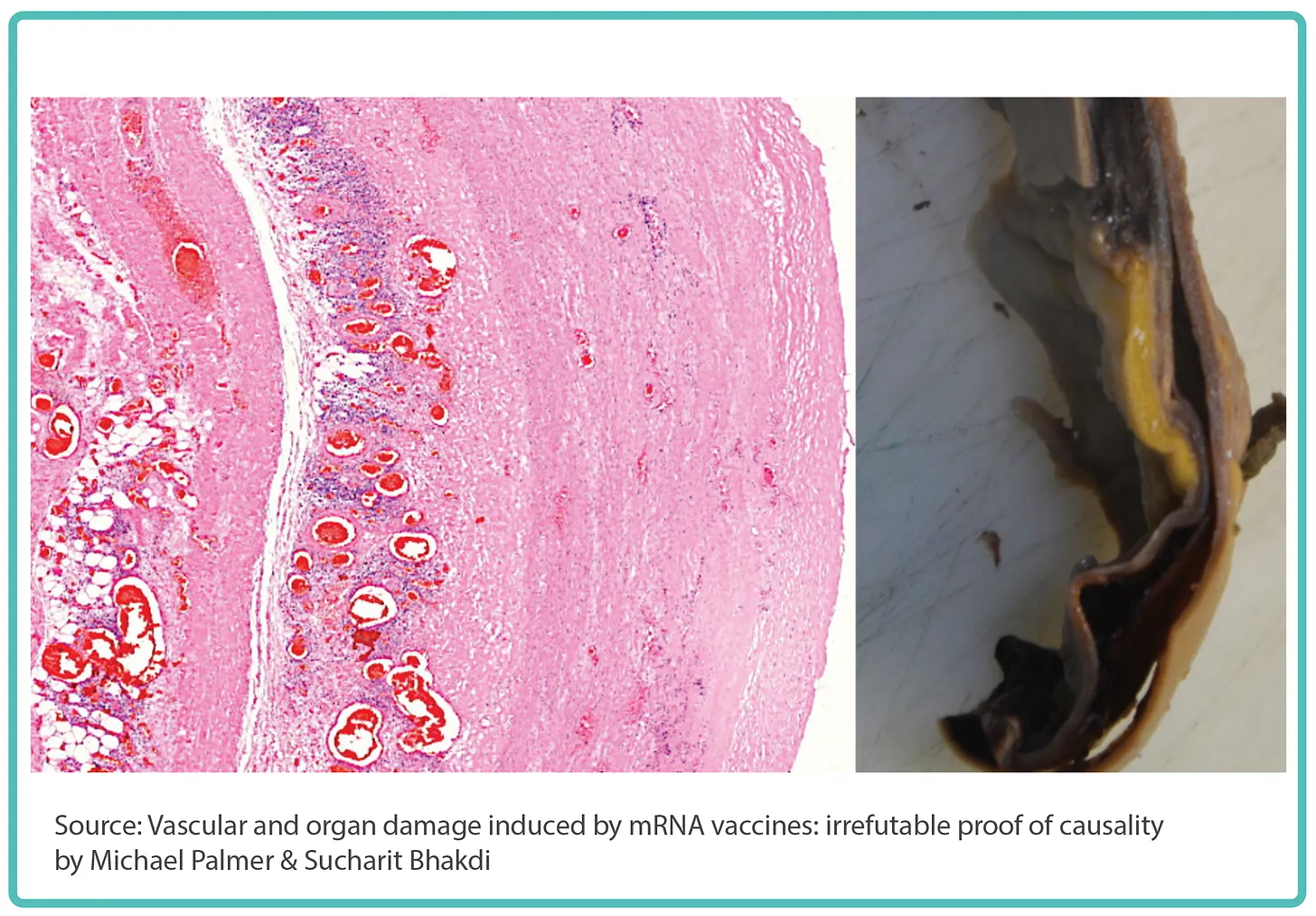
(A) Arterial Damage + (B) Deep Vein Thrombosis 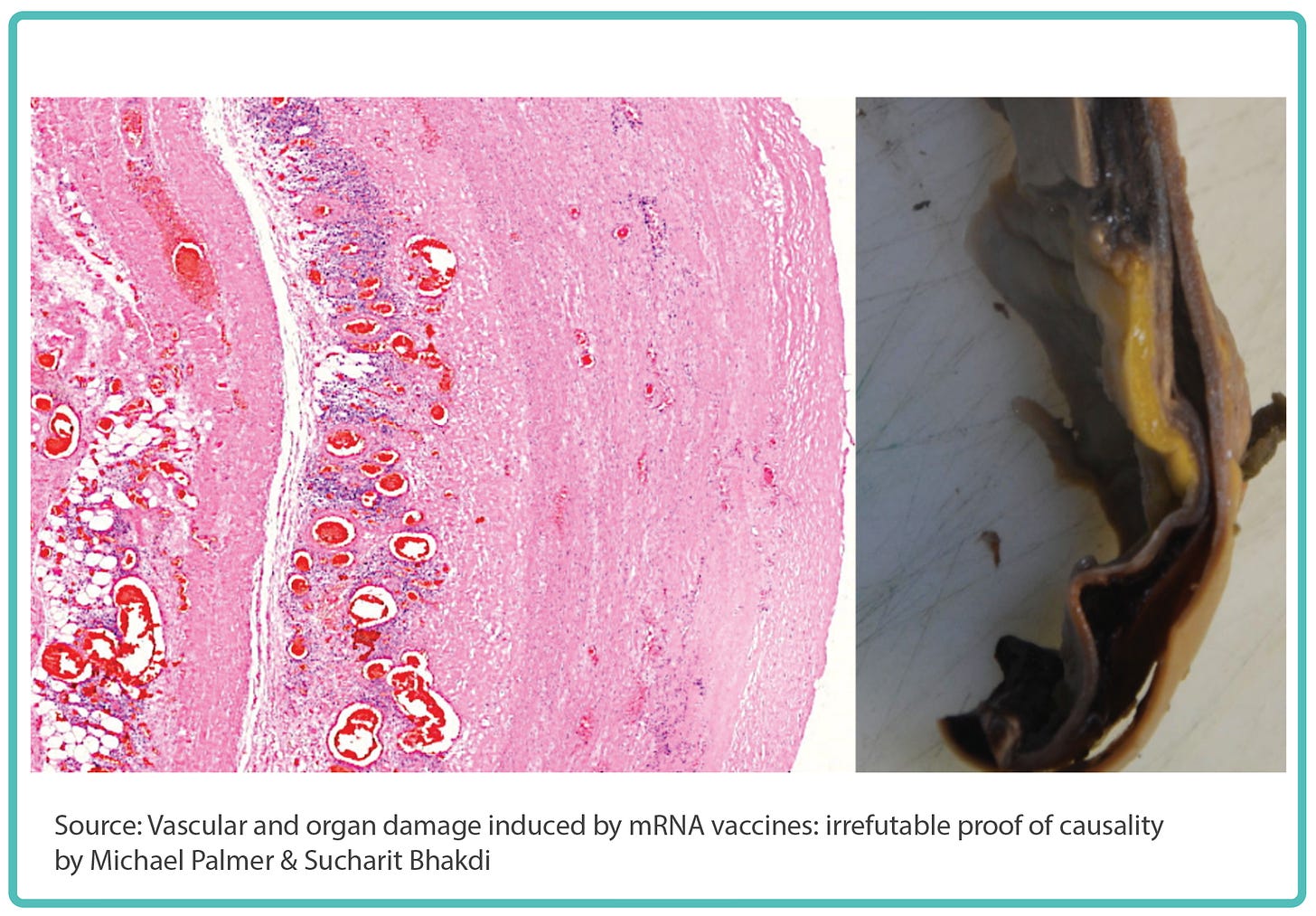
A crack in the wall of the aorta, lined by lymphocytes, leading to aortic rupture. This is what Pr. Burkhardt in Germany has witnessed in many of his autopsies.
This is also consistent with the white material extracted from the arteries of many cadavers and patients this past year. This is also in line with the findings27 of a team at the Karolinska Hospital in Stockholm Sweden that found many deep-vein thrombosis28.
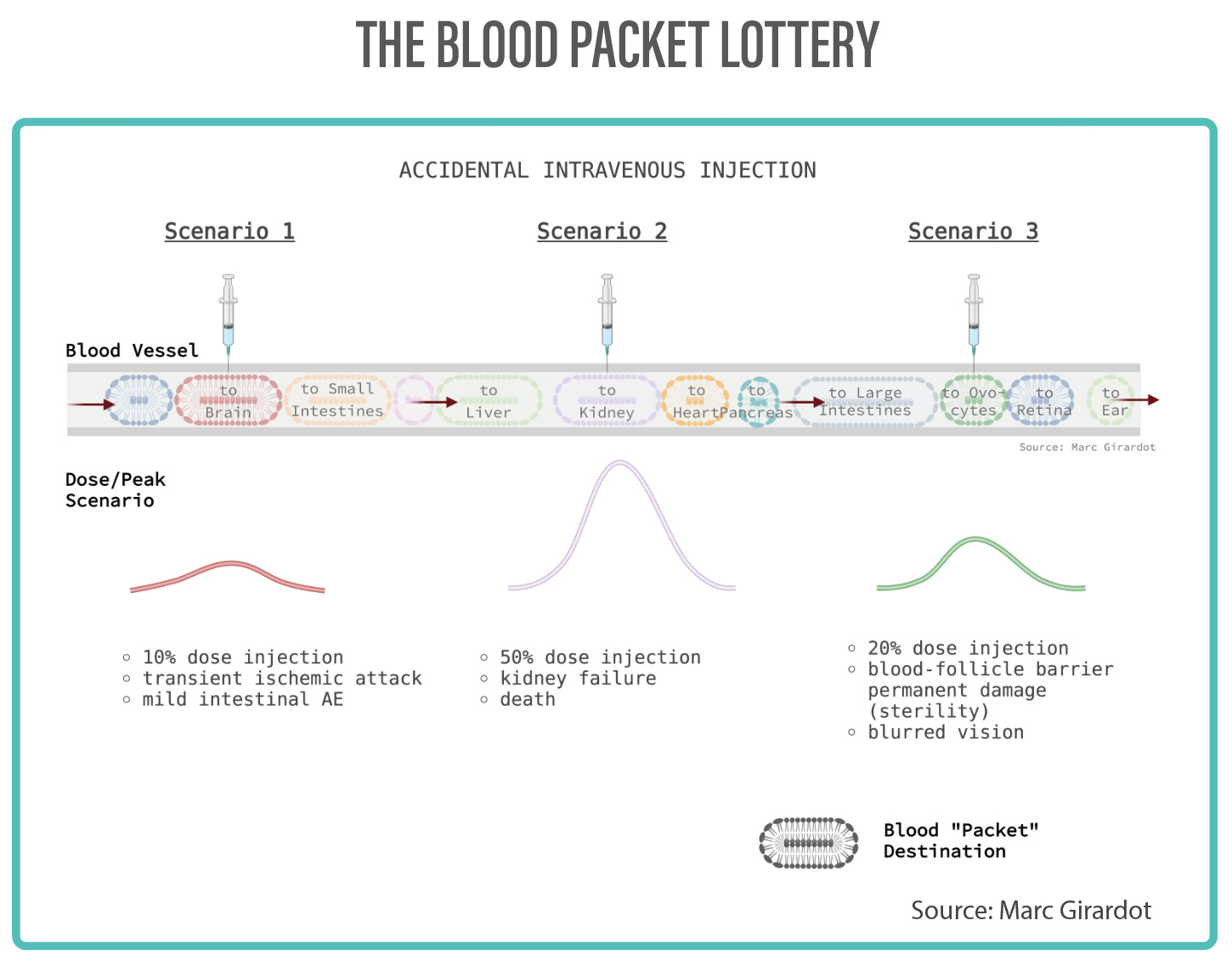
Past the heart, the aorta, and downstream from the arteries, when the capillary topology becomes tighter, the probability for transfection also is great, but the dilution means that the bolus is slightly less potent. Depending on the timing and the location of the shot, it is likely that a specific place, or a few specific areas will be at risk of a clustered transfection: not sure we can ever simulate that. But, like if you were to intercept a IP packet on a Internet network, there’s a lottery of blood packets (similar to IP packets) destined to more or less life critical organs.
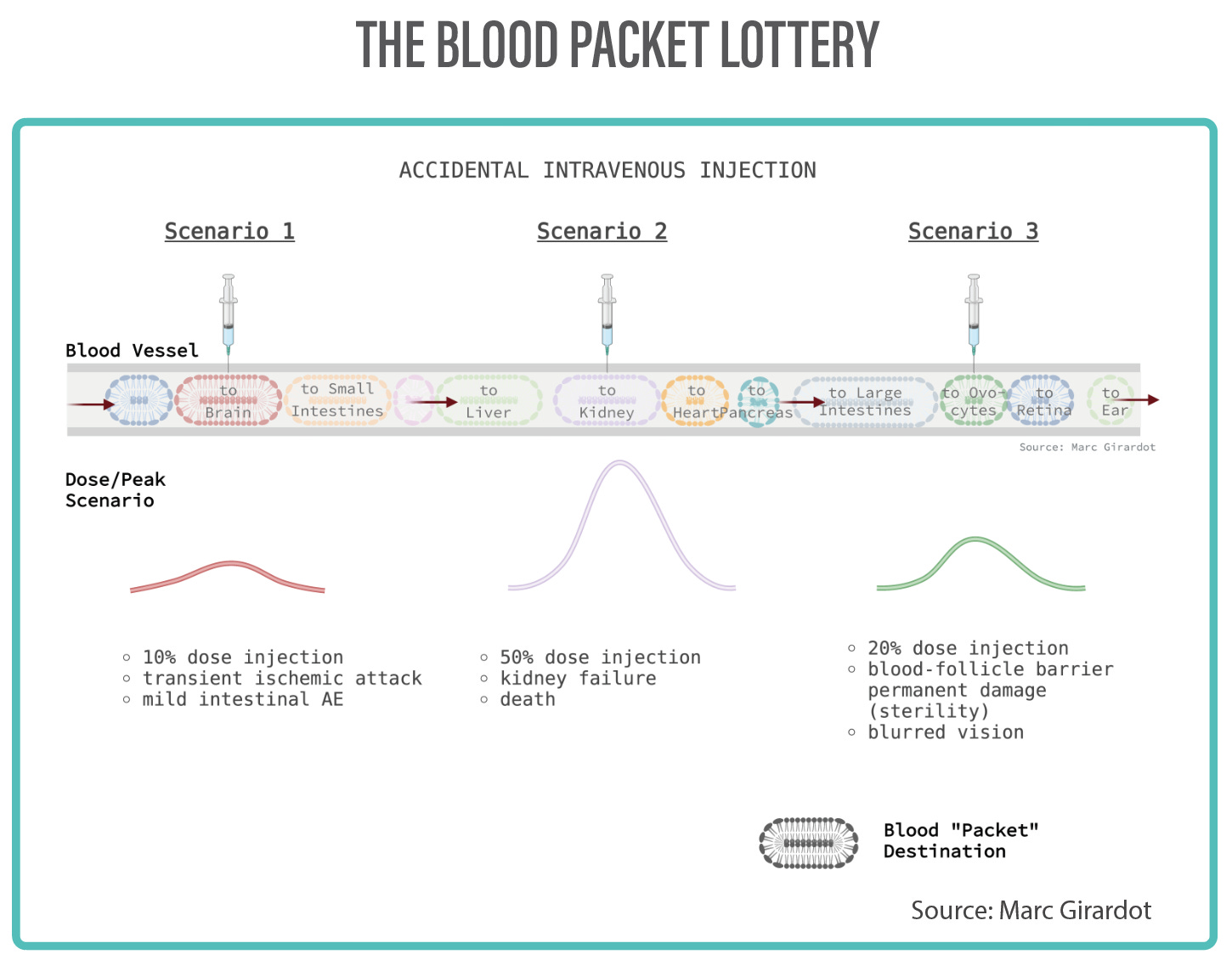
In these organs, large or small, life-critical or less critical, varying degrees of transfection will cause varying degrees of inflammation, clotting, of downstream necrosis, and occasionally organ failure (SADS, SIDS).
In the case of my friend, this likely occurred in the lungs where 30% of his pulmonary capillaries got clotted and ended killing his alveoli. It is possible clots from the lungs ended up in his heart.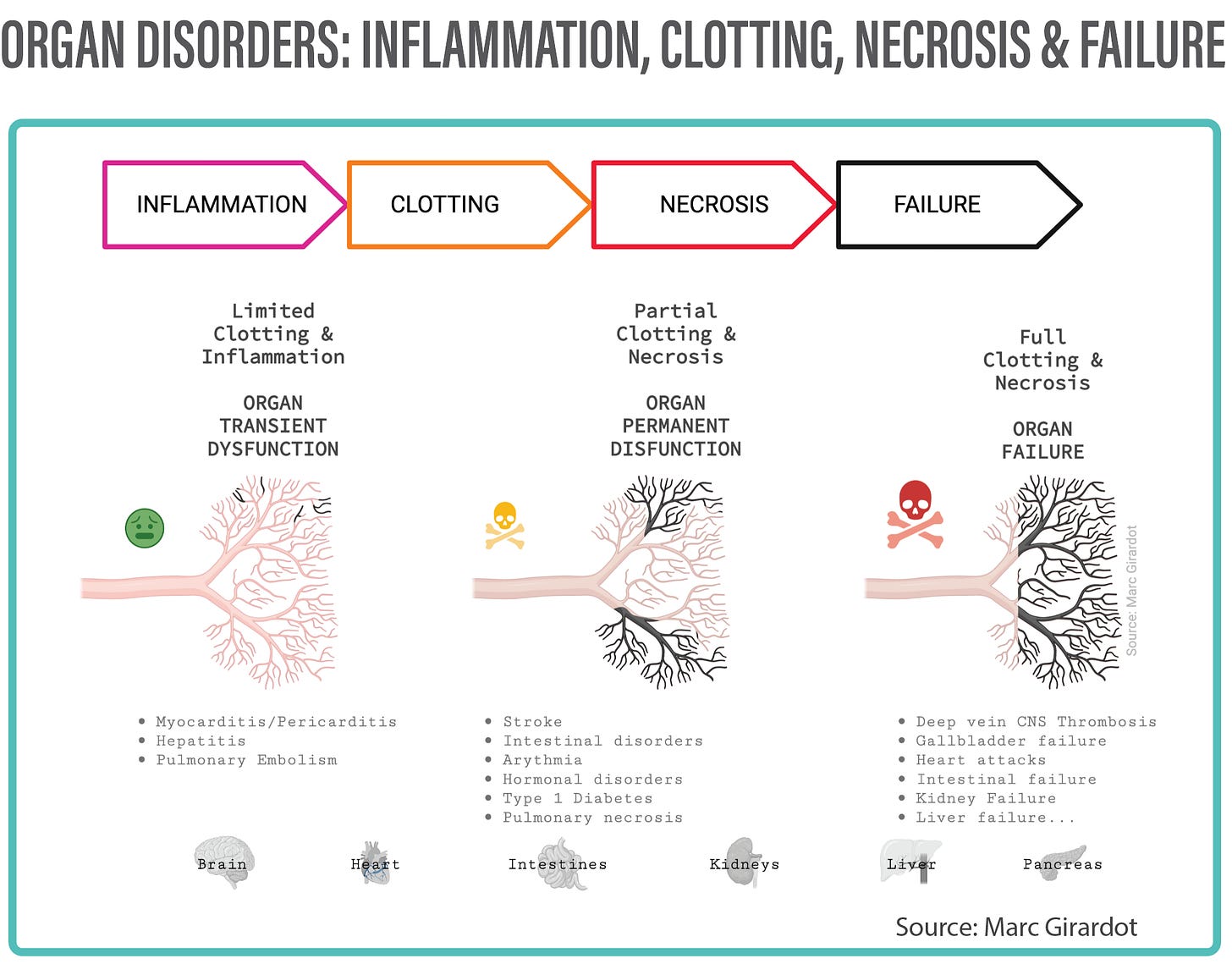
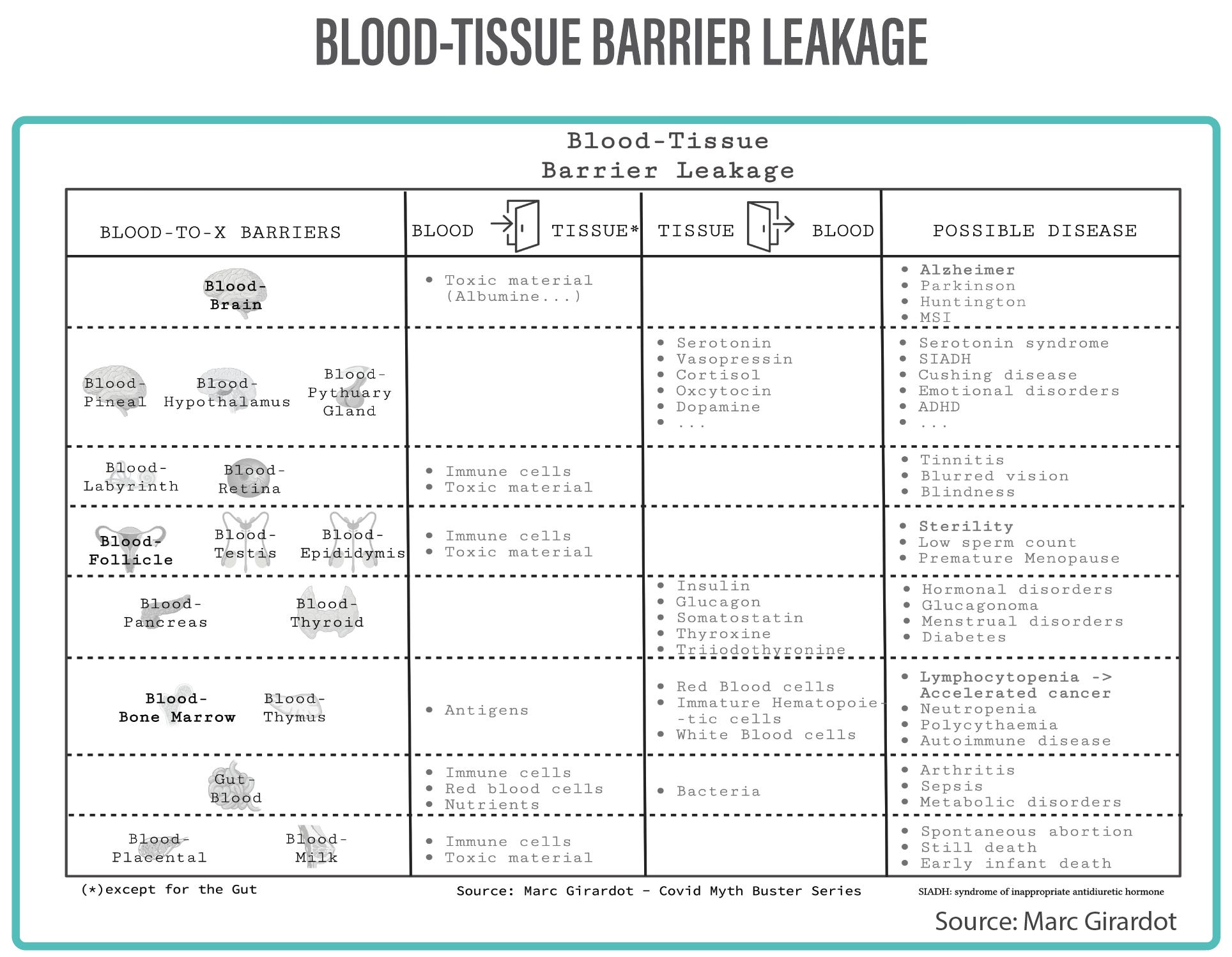
(C) Organ Inflammation, Damage & Failure In a number of organs, the endothelium plays a critical regulating role: The blood-tissue barrier stops toxic elements and immune cells from entering and causing damage, or regulating cells and hormones produced in the organ.
If the endothelium is damaged sufficiently, it won’t be in a capacity to plays its role. Imagine if you couldn’t close your door: your kids could go out and escape, or anyone would be able to come in eat your lunch or drop some garbage in your living room. That’s what happens when the endothelium is damaged :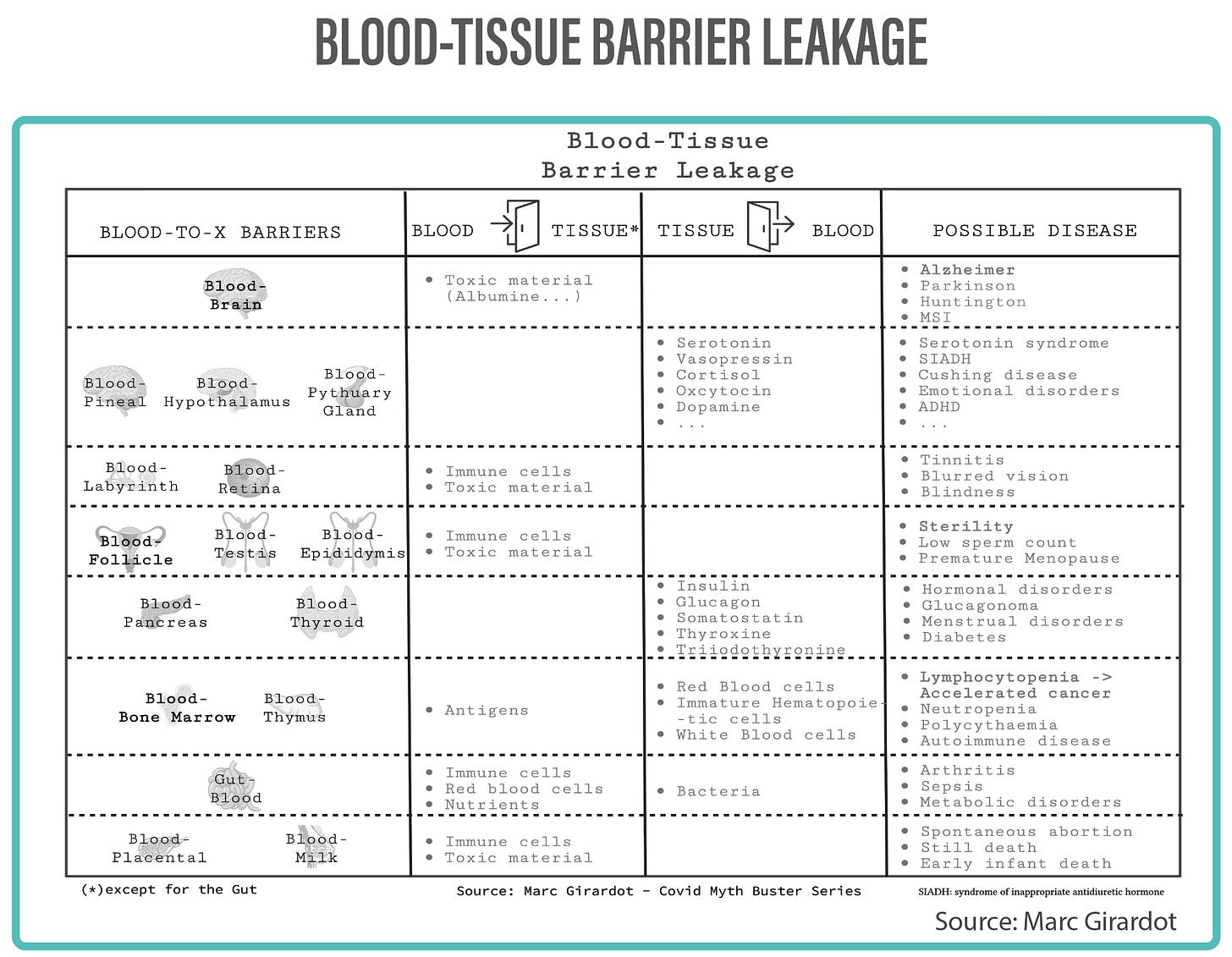
if the blood-bone marrow barrier is open, immature immune cells can escape into the bloodstream spoiling a great part of the immune cells produced, diminishing greatly its capacity: explains reappearance of dormant shingles and more importantly the recent increase in fulgurant cancers. With limited T-cells (Lymphocytopenia) to fight tumour growth, cancer can become lethal very rapidly.
It could also explain Polycythaemia, supposedly producing too many red cells…but in reality, it is very reasonable to think that Vaquez disease is due not to overproduction of red cells, but to uncontrolled liberation of red cells into the blood by a leaky blood-bone marrow barrier.
Similarly, if hormone controlling barriers are breached: hormone producing organs can leak hormones constantly creating hormonal disorders such as Cushing, SIADH, Diabetes, ADHD, Prolactinoma … Many theories point to over-production of hormones or cells, could well be the gate is simply open and hormones are flowing out uncontrollably.
I have already mentioned in “Poking Holes in the Brain-Blood Barrier. Is that such a good idea?” the serious neurodegenerative implications of a leaky brain-blood barrier. The clinical signs of accelerated dementia only confirm that the theory is well founded. It is reasonable to think that accidental iV injection can lead to a new wave of Alzheimer Disease.
The implication on the reproductive system also are severe. I had addressed that in: “Can Vaccines be Dangerous to Pregnant Women, Babies and Human Reproduction ? - A Credible Mechanism of Action”. The blood-follicle barrier protects ovocytes, and the blood-testis and blood-epididymal barriers protect spermatozoids, from toxic material and immune cells. If breached permanently that could mean sterility.


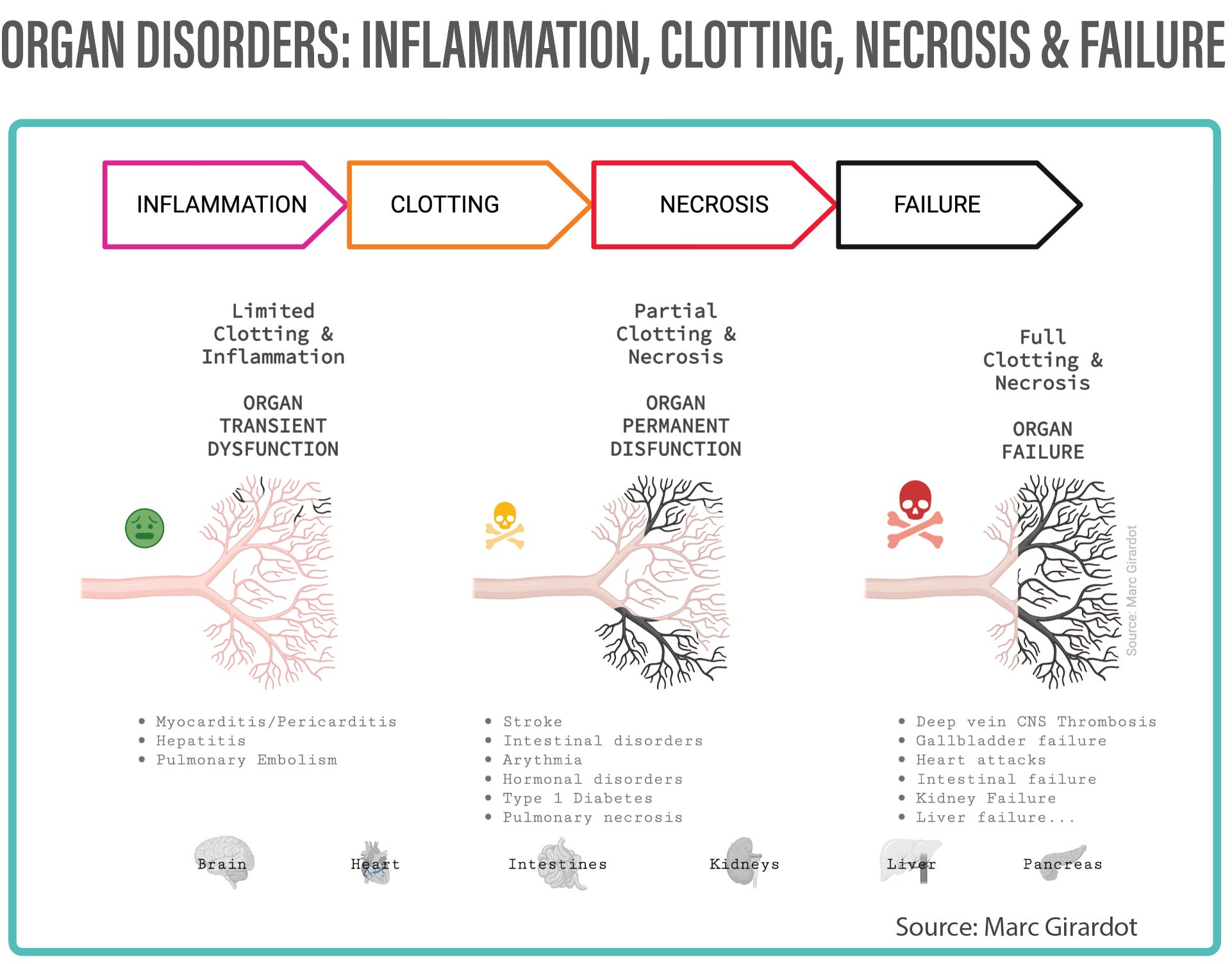
To summarise, the Bolus Theory stands on very solid ground: clinical, theoretical, physical and experimental, and is not limited in its scope to COVID vaccines. The type of pathologies triggered by an injection of a transfecting vaccine intravascularly are:
A. Arterial damage leading to further artherosclerosis, and in the most severe cases arterial rupture, haemorrhage and death.
B. Clotting and deep-vein thrombosis caused by significant endothelial damage int he arteries.
C. Organ inflammation, dysfunction or failure due to varying degrees of localized immune attacks in the capillaries.
D. Blood-tissue barrier leakage, transient or permanent, that can a variety of illness depending on the organ’s sensitivity to blood elements (brain sensitivity to albumine for example), or the implication of uncontrolled elements produced by the organ such as red blood cell, immature immune cells or hormones.
Earnestly, the evidence is quite compelling. I know some would like more sophisticated genetics-based or microbiology-based scenarios.
Frankly I don’t understand why dentists, anaesthesiologists, plastic surgeons and many other players in the medical field would be subject to drastically strict measures to avoid intravascular injection accidents, and we would not care for a procedure rolled out to billions!?
I hope you enjoyed this piece, and that it will finally have a positive impact to help us get out of this nightmare. Feel free to reach out.
Love.
Marc

“What happens to those billions of NanoParticles you've become host to?” by Marc Girardot
“Frequency of accidental intravascular injection of local anaesthetics in dental practice” by Anthony M.Schiano
“Management of a Vascular Occlusion Associated with Cosmetic Injections” by Martyn King
“Efficacy of Retrobulbar Hyaluronidase Injection for Vision Loss Resulting from Hyaluronic Acid Filler Embolization” by Guo-Zhang Zhu et al
“Accidental Intravascular Local Anesthetic Injection of the Facial Artery” by Matias Garcia-Blanco
“Accidental Intra-Arterial Injection: A Hazard of Intravenous Medication” by Richard G.Topazian
“The role of accidental puncture of veins in the production of allergic shock” by G. L. Waldbott - 1936
“Frequency of accidental intravascular injection of local anesthetics in dental practice” by
Anthony M.Schiano et al
“Dry cough after testosterone undecanoate injection: A case report” by Roberto Vita
“Inadvertent subcutaneous injection of COVID-19 vaccine” by Jia Yu Ng
“Recurrent injection-site reactions after incorrect subcutaneous administration of a COVID-19 vaccine” by M. Gyldenløve
“A Prospective Study of the Incidence of Myocarditis/Pericarditis and New Onset Cardiac Symptoms following Smallpox and Influenza Vaccination” by Renata Engler et al
“Natural killer cell-mediated ADCC in SARS-CoV-2-infected individuals and vaccine recipients” by Kerri Hagemann et al
“Role of the antigen presentation process in the immunization mechanism of the genetic vaccines against COVID-19 and the need for biodistribution evaluations” by P. Polykretis
“Induction of shock after intravenous injection of adenovirus vectors: a critical role for platelet-activating factor” by Zhili Xu
“Pericarditis with Increased Vascular Permeability after COVID-19 Vaccination” by Tadao Aikawa et al
“Metal taste side effect reported after Pfizer Covid-19 vaccination” - NBC News March 25, 2021
“Accidental IV injection is real: Ever heard of "Tren Cough"? Bodybuilders regularly suffer this adverse event after steroid injections” by Marc Girardot
“A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following Smallpox and Influenza Vaccination” by Engler et al
“Poking Holes in the Brain-Blood Barrier. Is that such a good idea?” by Marc Girardot
“A Prospective Study of the Incidence of Myocarditis/Pericarditis and New Onset Cardiac Symptoms following Smallpox and Influenza Vaccination” by Renata J. M. Engler
“Complications of injectable testosterone undecanoate in routine clinical practice” by T.Middleton et al
“Andrology: Tolerability of intramuscular injections of testosterone ester in oil vehicle” by Mary-Anne Mackey
“Who in their right mind would play Russian Roulette with a critical organ? ” byMarc Girardot
“It's Not the Free-Floating Spike Causing Adverse Effects!- Vaccine Safety Myth - Data show that the spike is absent after jab2, how could it be the cause of the damage?” by Marc Girardot
Addendum: I had made a mistake in the number of LNPs, it was corrected back down to 10 and 40 bn, respectively for Pfizer and Biontech. Apologies.
“Intravenous Push Administration of Antibiotics: Literature and Considerations” by Samantha Spencer
“Thermography and plethysmography, a non-invasive alternative to venography in the diagnosis of deep vein thrombosis” by K. Holmgren et al
“Computerized Thermographic Imaging and Live Blood Analysis Post C19 Injection: Shocking New Images - Stop The Shots Now!” by Ana Maria Mihalcea, MD,