


Vaccine Russian Roulette : Why some might be just fine and some not...
Vaccine Safety Myth - A Probabilistic "Theory" on the Safety and Toxicity of Cell-Penetrating Vaccines

Last month in Australia, heavy rains forced operators of dams reaching capacity to release immense quantities of water downstream flash-flooding entire regions and threatening the lives of thousands.
It’s compelling to note the vivid contrast:
on the one side, a controlled progressive flow of water would have been invisible and harmless to a passerby, a charming chanting stream;
on the other side, a few hours later, the same amount of water uncontrolled descending brutally on a population and their houses becomes monstrous, life-changing and devastating.
The analogy with vaccines is more striking than one thinks: for many, these vaccines have proven to be safe, and to some - too many - they have proven harmful.
And I believe, it’s also a question of flow…

Today I demonstrate that:
Scuttling billions of cells repeatedly - outside the muscle -cannot be innocuous, and is likely the principal root cause of all the vaccine adverse effects witnessed.
This realisation means that current vaccine technologies, as well as mass vaccination techniques and processes, need to be audited and revisited rapidly, to account for these findings.
I want to thank whole-heartedly all the kind subscribers who have contributed generously and voluntarily.
Being recently unemployed, your voluntary help is welcome and deeply appreciated.
Apologies to all, this article is a bit technical at times and long , but it is an indispensable step to pinpoint the circumstances by which these vaccines can be dangerous.
Note: For the purpose of simplification, I will be using the term nanoparticle for any vaccine vector vehicle capable of penetrating a cell and delivering inside a foreign genetic load that includes mRNA/DNA vaccines, attenuated viruses and viral vectors.
For over a year now, I have been highlighting a fact that most “experts” have seriously been overlooking for the past decades:
All cells penetrated by nanoparticles, mRNA or viral vector, will necessarily be destroyed by the immune system
As you can see below in the description of the mechanism of action of an anti-COVID mRNA vaccine, the transfected1 muscle cell is supposed to die. That’s what apoptosis means. The destruction of all transfected cells is part of the process by which the immune system is stimulated, and it happens quite rapidly.
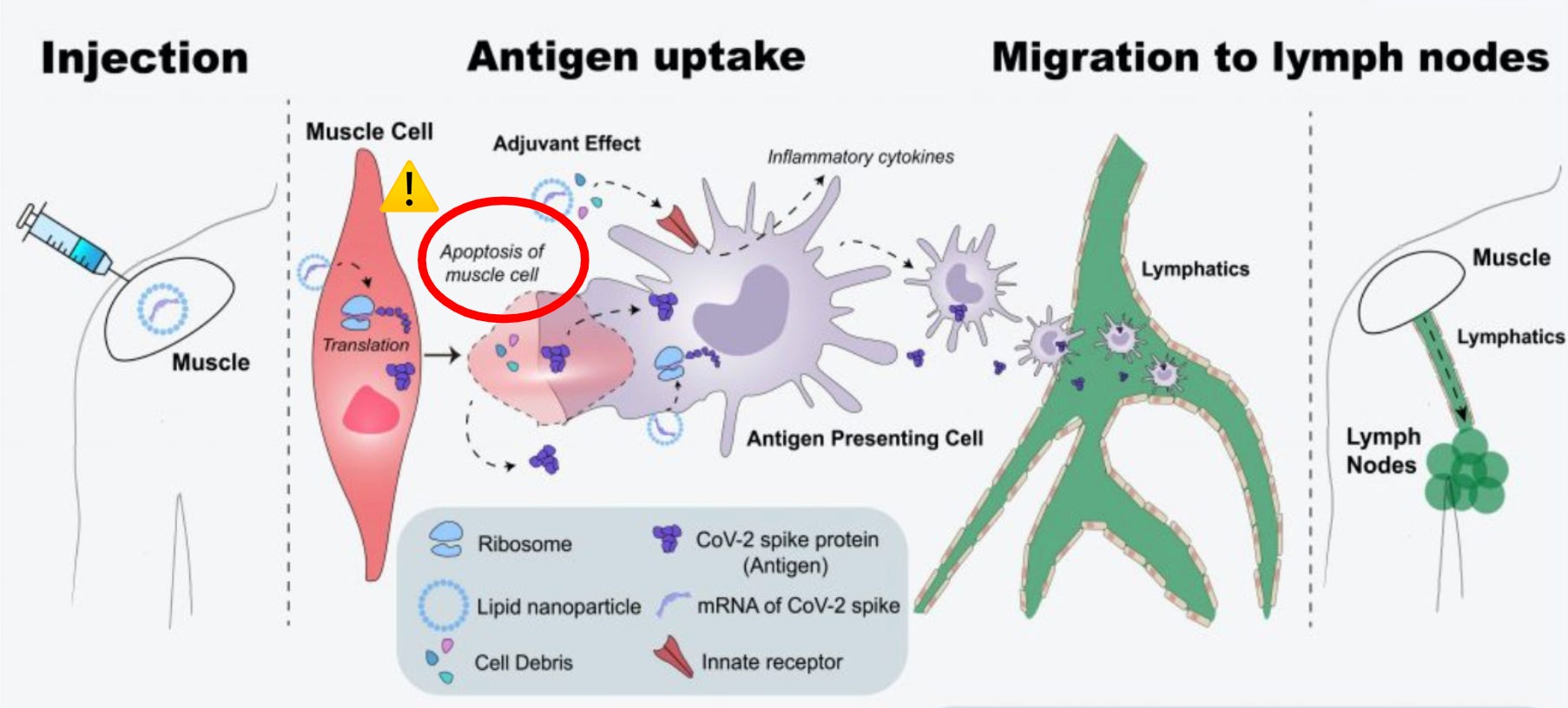
credit: T.Karginov
For the record, one has to remember that these technologies were adapted from anti-cancer technologies with the very purpose of stimulating T-cells and destroying tumour cells. So, it should not come as a surprise.
Vaccine designers re-purposed these platforms to trigger transfected cell destruction to liberate spike proteins into the tissue so that they can be processed by immune cells and stimulate the production of antibodies.
In layman’s terms, pre-booster vaccination meant every future Vaccinated agreed to have up to :
30 billion cells scuttled for a Pfizer-only combo
80 billion cells destroyed with 2 shots of Moderna, and
100 billions cells wasted by 2 shots of AstraZeneca!
To be honest, in principle, that should not have been a problem because these cells were supposed to be muscle cells which can regenerate.
On paper, the vaccines should have been relatively innocuous.
Can nanoparticles end up in the blood stream?
I have already addressed extensively in previous articles on the leak from the muscle, and on the risk of intravenous injections.
If nanoparticles escape the muscle - which is clearly proven from the Pfizer data - the circulatory system inevitably becomes their receptacles, and LNPs will start doing what they were designed to do: transfect, penetrate endothelial cells in very large numbers.
It is noteworthy to highlight that what is true for mRNA and DNA vaccines, is likely also true for viral vectors and attenuated viruses vaccines.
German pathologist, Professor Arne Burkhardt, recently told us that up to 5% of direct intravenous injection can occur. Though that seems a frighteningly high number, physiologically that’s certainly a possible proportion.
Injection Needle Tip vs Blood Vessel Size
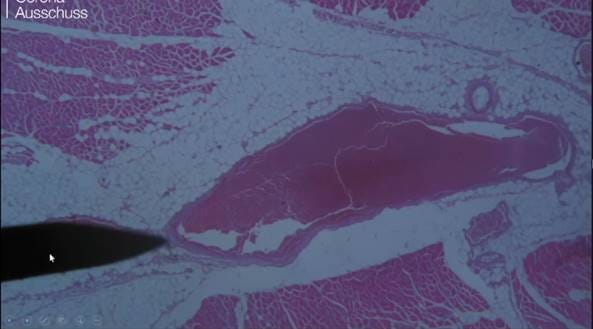
Credit: Prof. Dr. Medical Arne Burkhardt
The above picture extracted from Pr. Burkhardt’s latest report demonstrates the physical possibility of a partial or total injection into a blood vessel.
Depending on local training, local protocols and the quality of the medical personnel in charge of vaccinating this necessarily would vary widely.
Literally Russian Roulette !
Why are some injections less dangerous than others?
Let’s do the math!
10 billion nanoparticles spread over 100,000 km of blood vessels,
that’s theoretically destroying 1 endothelial cell every centimeter.
Indeed, that shouldn’t be cause for alarm2.
And that’s likely what happens with many vaccinated folks who have had no issue: The nanoparticles are distributed enough that transfection zones are scattered throughout the endothelial surfaces of the body and the micro-environment balance - the homeostasis - is not disrupted significantly to start a domino effect. A neighbouring cell to the one sacrificed on the altar of immunisation rapidly divides and substitutes back in place a new cell.
If the hits on endothelial cells are highly concentrated, the endothelial wall will be devastated, smooth muscle cells exposed and damaged, and the whole balance of the blood vessel tipped towards clotting, crystallisation and necrosis. Not good.
All adverse effects seem tightly correlated to this deleterious process, either as a micro or a macro event…
In other words, to be innocuous, cell-penetrating nanoparticles need to be diluted so that the probability of concentrated hits is inexistent.
To come back to the “Dam and Water Analogy” , if the water flow is controlled, the shock is absorbed in time and in space, and balance can be maintained. If not, the flow will cause chaos and death in unfathomable ways.

Outside the muscle, where have vaccine nanoparticles the highest probability of penetrating and harming?
The Blood Vessel Diameter Factor
Here the data is extremely clear.
First and foremost capillaries and arterioles will inevitably be transfected most for probabilistic reasons tied to their diameters. The smaller the diameter, the greater the endothelial exposure relative to blood content. This makes perfect sense as it’s the zone where nutrients are delivered to cells.
Based on surface/volume ratios within blood vessels, a single vaccine nanoparticle has a 1,000 times more probability of encountering endothelial cells in the capillaries than in the arteries.
To a certain extent, this logic is similar to the concept to temperature loss: when animals regroup together in the blizzard, they limit their surface/volume exposure, and can collectively withstand the cold. In the vaccine context, the larger the blood vessel, the smaller the probability of concentrated transfection and harm, everything else being equal.

The NanoParticle Concentration or Dilution factor
The relative size of a lipid nanoparticle to a capillary at its smallest is about 1 to 100…
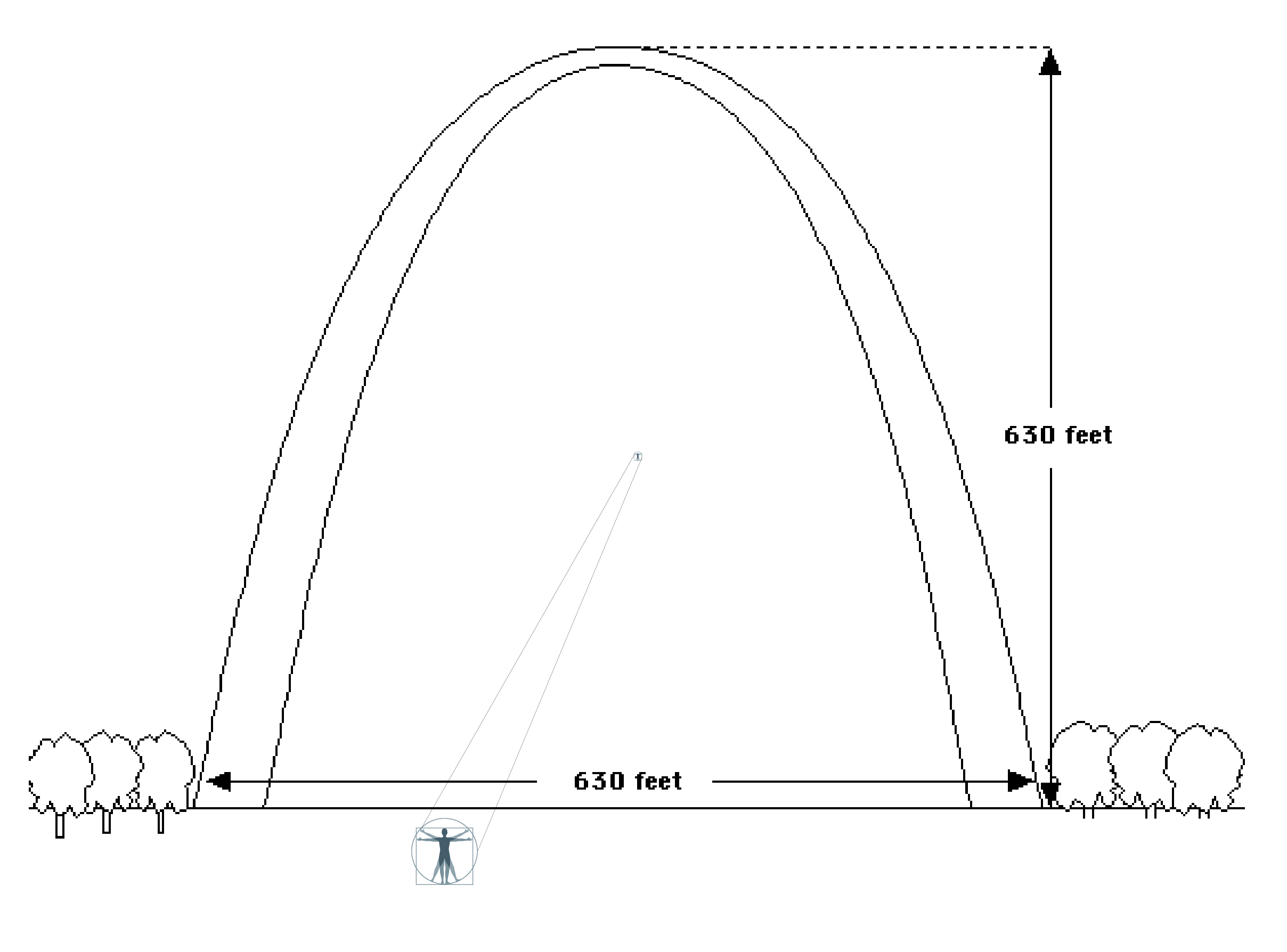
… about the same proportion as a man standing under the Great Arch of St.Louis. As you can see the probability of meeting the wall is very very low…
Concentration of vaccine nanoparticles in the blood inevitably plays a key role, notably in the few minutes after injection when it’s not yet diluted. Indeed, only when concentrated, will the vaccine vectors be in a large enough number to systematically hit a concentrated area.
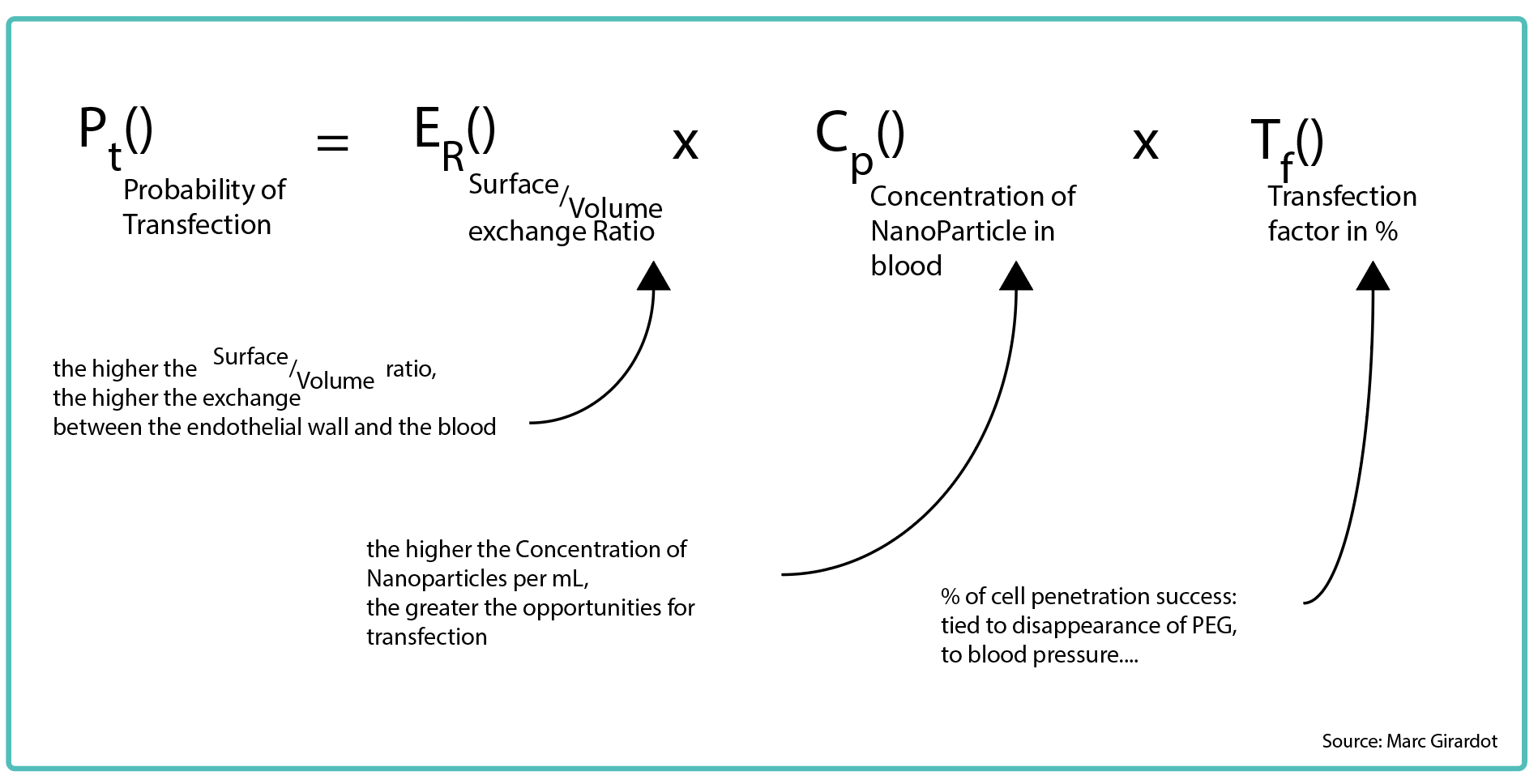
For transfection to occur the nanoparticle needs to meet with the endothelial wall, that is a function of blood vessel diameter as stated above, of concentration in the blood stream, and of a transfection factor (pressure probably plays a role pressing the nanoparticle onto the cell, PEG wearing-off also…).
In other words, only in the tiniest of vessels and during the first few minutes - before full dilution into the blood - will these injections have a probabilistically meaningful opportunity to transfect endothelial walls in a concentrated dangerous fashion.
Logically, intravenous-delivered drugs are generally injected very progressively - over a full minute - to avoid such concentrations in their delivery. This practice supports greatly my theory. A dose injected intravenously could translate to a concentration of 143 million3 LNPs per mL, versus 2 million LNPs per mL if done progressively.
In other words, during those few brief instants, transfection intensity can be enhanced 70x, and 1,000x versus a progressive leak following an intramuscular shot.
Why Virus-induced Myocarditis Can Never be as Bad as Vaccine-Induced
Following this logic, casual Covid-triggered myocarditis can never be as bad as myocarditis caused by vaccines. Indeed that would require the same homogeneous and simultaneous transfection of cardiac blood vessels. That can only be mathematically possible with:
an enormous amount of infected cells…
liberating billions of virions
directly in the blood stream
at the exact same location, and …
at the exact same instant…
… else they would less be concentrated, be dispersed and infect more homogeneously throughout the body.
It is mathematically, chronologically and physiologically impossible to mimic that level of concentration at a precise location and at the precise timing.
Only a seringue in the hand of a time-pressured undertrained professional can deliver the concentrated level of cytotoxic load that can cause severe myocarditis.
What difference between intravenous and intra arterial injection?

Vaccine injured, mountain bike professional, Kyle Warner mentioned that he had a metal taste in the mouth immediately after injection.
The instantaneity and the multiplication of symptoms - pericarditis, POTS and reactive arthritis - indicate the nanoparticles had to be transported by the bloodstream and distributed throughout the body. It also suggests an intravenous injection of the vaccine in a vein upstream from the right subclavian vein.
Indeed an artery injection would have directed the particles towards the muscles, nerves and bones of the right arm and hand, starting to dilute nanoparticles into the blood and starting to transfect endothelial cells in muscles, bones and nervous areas.
Most likely an intra arterial injection is innocuous in the muscle, but possibly damaging to nerves medium term with calcification following smooth muscle damage in blood vessels around nerves.
Dr. Stéphanie Senneff recently sent me an email she received from a vaccine injured suffering from calcific tendonosis, a likely consequence of an intra arterial injection..
Though such an injection would be far more dangerous than an intramuscular injection, it certainly would be much less dangerous than an intravenous one…
Into the Lungs
In the case of a direct vein injection of the Pfizer vaccine, the worse case scenario would be the entire dose of nanoparticles would land in the heart’s right ventricle and mix with 70mL of blood, and then get injected into the lungs with a concentration of 150-200 million LNPs per mL (make that 4x and 5x for Moderna and AstraZeneca!).
In the following table, I show that 98% of the transfection in the Lungs is bound to happen in the nearly 100 kilometers of pulmonary endothelial capillaries, arterioles and venules, where the blood to endothelial exchange is the highest.
If the PEG compound doesn’t prevent transfection at that moment (because of bad manipulation for example), the result would be necessarily disastrous, possibly causing massive pulmonary embolism.
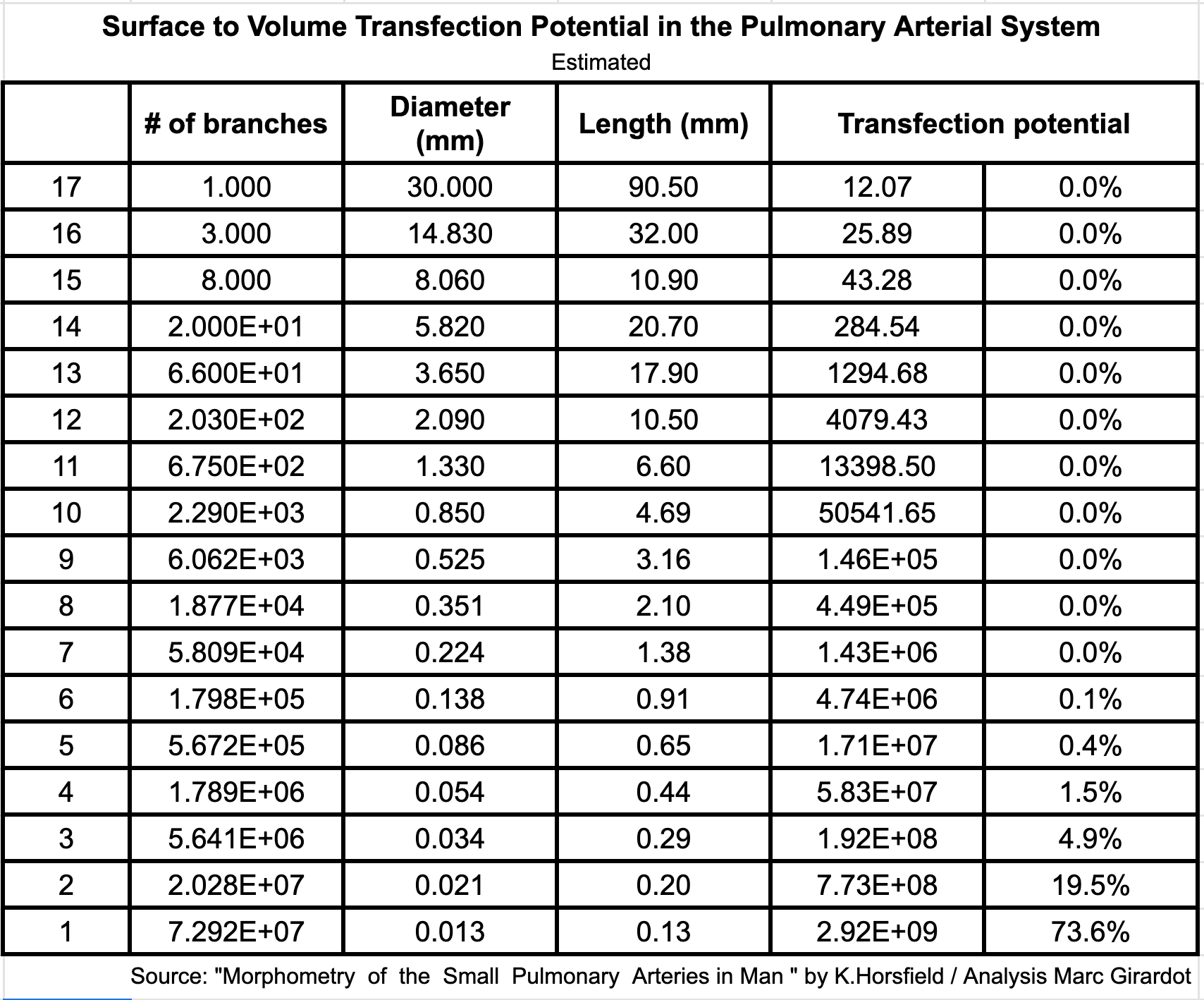
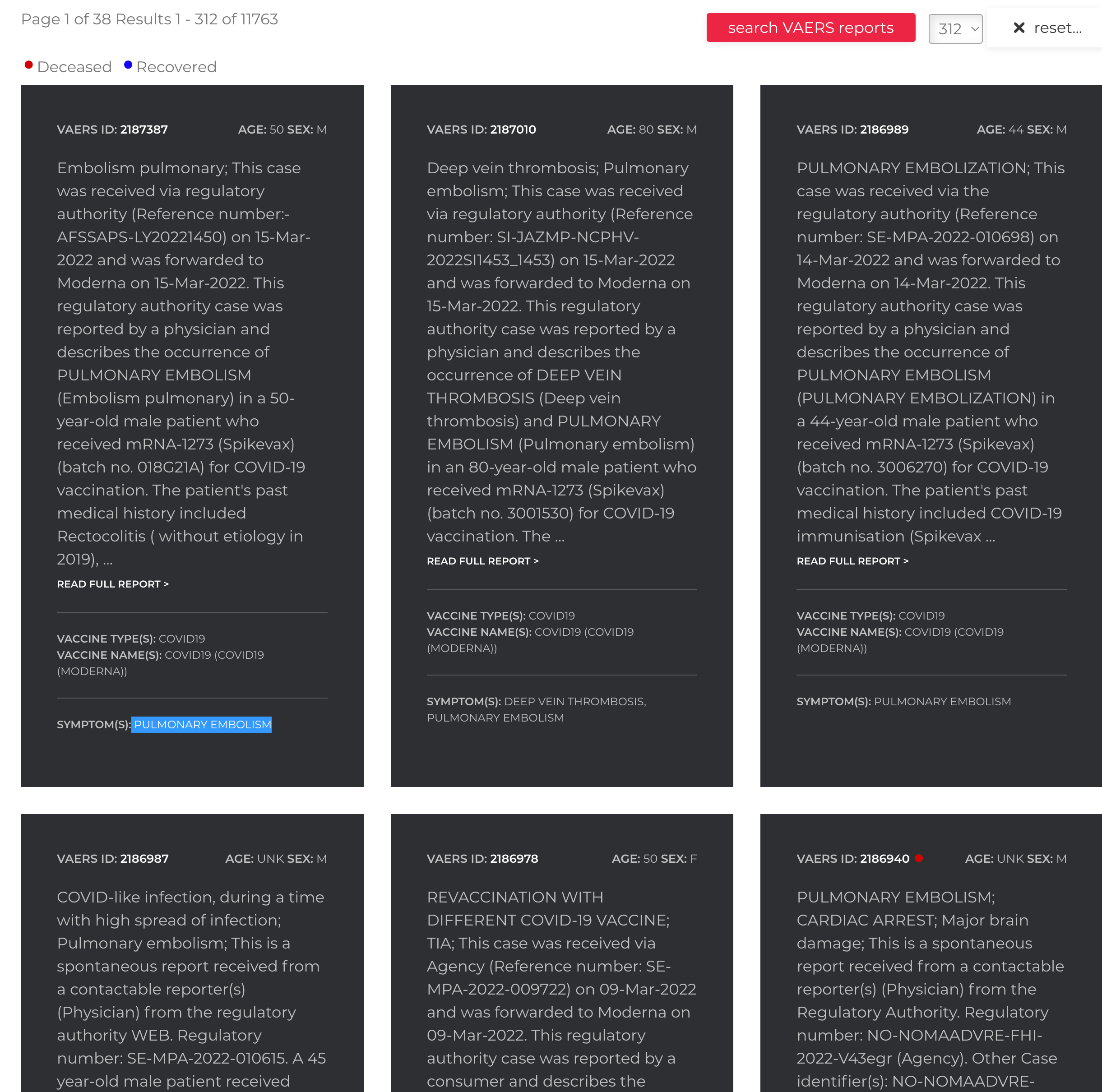
Consequently, it is not surprising to find 11,763 reports of pulmonary embolisms in VAERS.
Out of the Heart Into the Aorta
Past the lungs, the wider arteries, ventricule and aorta endothelial walls can be hit, but with an intensity divided by a factor of 1000 or more. However, it is plausible/realistic that transfection can be enhanced by the much higher blood pressure in the Aorta.
Recently, German pathologist, Dr. Burkhardt showed aortas could be damaged following vaccines with ultimately a collapse of the aorta. He declared:
“We have these focal textural disorders with the loss of elastic lamellae - and this is important - also lymphocytic infiltration.
Well, that could be a coincidence. That was a patient who had a vascular lesion for some reason.
But then we found it almost regularly. The more closely we looked, the more frequently we found cases where the aorta or arteries were also affected. “
Damaged Aorta Wall
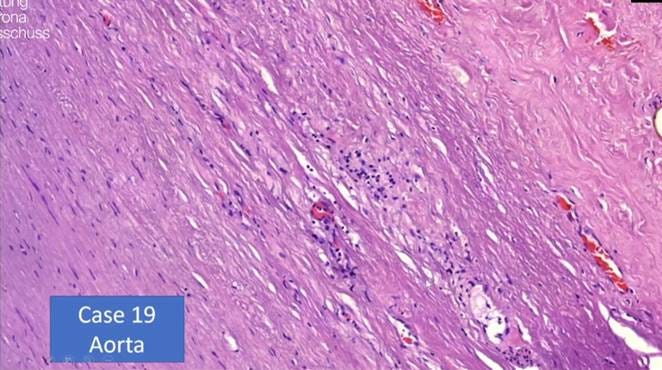
Credit: Prof. Dr. Medical Arne Burkhardt
The fact that the aorta and arteries downstream - more than veins - seem to be more at risk supports the hypothesis that, in higher blood pressure areas, nanoparticle penetration in healthy cells is enhanced, creating havoc in arterial endothelial walls and starting a degenerative - often lethal - process.
From the Aorta to Critical Organs
Past the Aorta, nanoparticles will start flowing with the blood intended to nourish critical organs heart, liver, brain, kidneys, spleen, ovaries… Obviously, the same dynamic will inevitably take place, as the arteries become arterioles and then capillaries, the transfection numbers will explode, and depending on where the highest concentration in nanoparticles ends up going, the greater the area of endothelial transfection will be.
Lymphocytes will then be recruited, will follow the same dynamic and hit with full force and destroy entire walls of these blood vessels. Bleeding and coagulation will follow … that will aggregate … cause more necrosis and harm behind, destroying valuable parts of the very organs the vessels were supposed to nourish.
This - in my mind - explains well the myocarditis and pericarditis, the thrombocytopenia and thromboses found across many vaccinated, heart attacks, strokes, as well as all the malfunctions of multiple organs we are witnessing post-vaccination. It also explains well the dichotomy between injured and not injured.
What about the Spike protein?
Many friends are convinced of the toxicity of the Spike protein. And frankly, there are biological grounds for that as I have written before.
So, please don’t shoot the messenger, les amis… :-)
Here’s the evidence that led me to believe the vaccine problem is more likely related to intravenous injections and to the cytotoxic effect of introducing foreign genetic material inside healthy cells than to the toxic effects of the Spike:
So far, many people simply have had no problem with the vaccine, that’s factual! Spike generation is common to everyone. If the Spike is the root cause, then why only a portion fall sick?
Studies have shown that T-cells can react very quickly - within a few hours - even if naive to the virus. That would support that Spike production is generally interrupted rapidly, and thus limited quantities of Spikes are produced.
The size of a spike protein is 9 to 12 nm, that’s 6,000x smaller than an endothelial cell, and 5,000x smaller than the vaccine nanoparticle. It can occasionally certainly bind to a receptor, but I doubt it can break or damage endothelial walls. Endothelial cell are designed by Evolution to resist being hit by a multitude of nano elements.
The ratio of a Spike protein to the tiniest capillary is 1 to 1,500. It seems completely improbable that these tiny elements would be in sufficient quantity in the blood to damage arterial walls as described above. The surface/volume conundrum becomes Himalayaesque given the nanosize of the Spike.
Even though, researchers have demonstrated presence of spike in tissues, even over time. I have yet to see a study demonstrating substantively wide presence of Spikes.
I have extreme confidence in the immune system’s capacity to identify transfected cells and to eliminate wandering Spike proteins. As such there is no reason to believe healthy individuals would not be able to contain the toxicity of the Spike, nevertheless many healthy individuals have had adverse effects.
Vaccine pathologies don’t concern only elderly and immunocompromised. One could have proposed that immunocompromised respond slowly and therefore produce obscene quantities of Spike. I have made that argument before. And it might happen, however that is absolutely not consistent with the diversity of profiles of the victims of the adverse effects. This is demonstrably not related to immune deficiency and a cascade of Spike.
Finally, the logic endothelial wall destruction by T-cells following their transfection is imparable and consistent with most, if not all, of the adverse effects symptoms.
In conclusion, it is imperative that Public Health authorities throughout the world acknowledge the dangers of intravenous injections of these vaccines, immediately review injection protocols and materials used to strictly avoid any rapid concentrated injection of these vaccines into the bloodstream.
The fact that the FDA, the CDC, as well as the European Pharmaco vigilance agency have been blind for over a year to the harm caused by the reckless vaccination processes rolled out in haste is absolutely intolerable. A complete overhaul of these organisations needs to happen.
Hopefully, collectively we will learn from this disaster, improve vaccine technology and emphasise on the criticality of the vaccination process: it is a medical intervention, and even the slightest detail can be deadly.
penetrated by vaccine nanoparticles
200+ neighbouring endothelial cells can easy replicate and substitute for the lost transfected cell
dilution occurring in the 70mL right ventricle